Access to services
Specialist palliative care tended to be first received in the last few weeks of life, driven by referrals to inpatient SPC
Consistent with the results presented in Receipt of care, SPC services in the last year of life for a population in need of palliative care was generally first received within the last few weeks of life – median number of days from receipt to death was 18 days (see Figure 4.5). This is driven by those in inpatient care as opposed to other settings, where there is a short duration between when SPC is first received in inpatient care and the person’s death (median of 10 days). 80% of the population in need of palliative care received SPC as inpatients.
It is likely that most people who first received inpatient SPC died during this admission, given that 67% of deaths occurred in hospital and 56% last received inpatient care in the last week of life (see Access). This may reflect that the population in need of palliative care are more likely to be referred to inpatient SPC in the last days of life than other settings. As shown in Figure 4.5, SPC referrals to community-based services (through MBS claims or outpatient clinics) occurred much earlier than for inpatient care. In outpatient clinics, the median number of days between when SPC was first received to death was 65 days; this was 47 days through MBS palliative specialist consultations, and 10 days where SPC was first received as inpatients.
First consultations with palliative care specialists occur on average 6 months later than with other specialists
On average, first consultations with palliative care specialists tended to occur 6 months after consultation with other specialists. Consultations with disease-specific specialists generally reduces (except for oncologists and nephrologists) in the last 3 months of life.
For the population in need of palliative care, the median number of days from first MBS consultations with palliative care specialists to death was 47 days (or within 1.5 months before death). This generally occurred at least 6 months after first consultations with disease-specific specialists in the last year of life. The median number of days from first MBS consultations with oncologists to death was 273 days (9 months), cardiologists 240 days (8 months), nephrologist 234 days (7.7 months), neurologists 221 days (7.3 months) and respiratory physicians 210 days (6.9 months). First consultations with geriatricians tended to occur slightly later, around 172 days (6 months) before death.
In the last months of life, consultations with these disease-specific specialists generally reduces – last consultations with cardiologists, neurologists and respiratory physicians occurred at least 3 months before death (median of 107 days, 113 and 106 days, before death, respectively), while last consultations with oncologists, nephrologists and geriatricians occurred closer to death (median of 38, 74, and 71 days before death). Palliative care specialists tend to be the last specialist to see a patient before death and this generally occurred in the last weeks of life (median of 8 days before death), as shown in Figure 4.5.
Note that these data reflect where an MBS claim has been submitted for consultations with specialists and does not capture informal discussions between palliative care and other specialists regarding the management and treatment of their patients with complex conditions. Evidence suggests that integrating palliative care services with disease-related care to provide multidisciplinary care can achieve better outcomes for people with complex life-limiting conditions (Palliative Care Therapeutic Guidelines).
First contact with GPs in the last year of life for the population in need of palliative care was close to the start of that year (mean of 348 days before death), and last contact was 7 days before death. This is expected as GPs typically act as the first point of contact for patients and play a key role in diagnosis, treatment, and management (including coordination of care with specialists and other healthcare providers).
Figure 4.5: Median number of days from receipt of first or last service to death, by type of service received, for population in need of palliative care
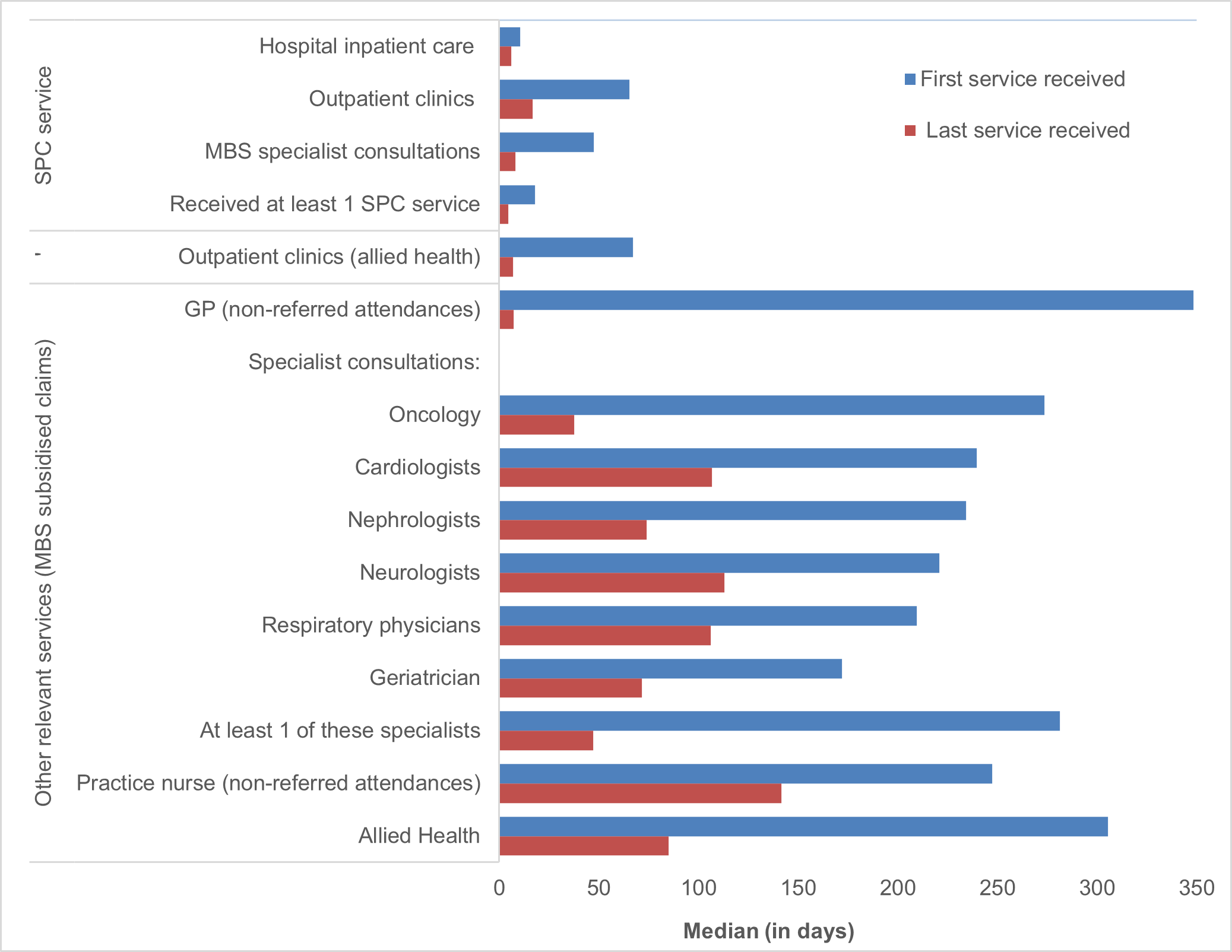
Source: Supplementary Table 6a.
SPC received earlier for cancer patients than for other end-of-life disease trajectories, particularly people dying from frailty
Examining when a service was first received by the end-of-life disease trajectories reveals some interesting patterns. As mentioned in Section 3.2, the population in need of palliative care dying from cancer tended to first receive SPC 3 weeks earlier than people dying from organ failure and frailty, 31 days compared with 8 and 6 days respectively, as shown in Receipt of care: Figure 3.5.
First attendances with GPs and practice nurses and receipt of allied health services in the last year of life were relatively similar across the end-of-life disease trajectories for the population in need of palliative care (see Supplementary Table 6b). However, some notable variations across the disease trajectories were observed for first MBS consultations with specialists, as shown in Figure 4.6.
As discussed in Access, people dying from cancer had first consultations with palliative care specialists in outpatient clinics and through MBS much earlier than people dying from organ failure and frailty – median number of days from first receipt of MBS palliative specialist consultations to death of 52 days for cancer compared with 31 days and 10 days, for organ failure and frailty. Corresponding medians for outpatient clinics was 76 and 52 days for cancer and organ failure. However, cancer patients tended to first consult with all other specialists (except oncologists) later than people dying from organ failure, as shown in Figure 4.6.
This analysis also highlighted that people dying from frailty were more likely to consult with geriatricians and neurologists earlier than people dying from other causes. They were also more likely to receive their last SPC service closer to death. Last consultations with palliative care specialists occurred 2 days before death compared with a median of 8 and 9 days before death for people dying from organ failure and cancer. Similarly last consultations with GPs occurred 1 day before death compared with 7 and 13 days before death for organ failure and cancer patients (see Supplementary Table 6b).
Figure 4.6: Median number of days from receipt of first consultations with GPs and specialists to death, by disease trajectories, for population in need of palliative care
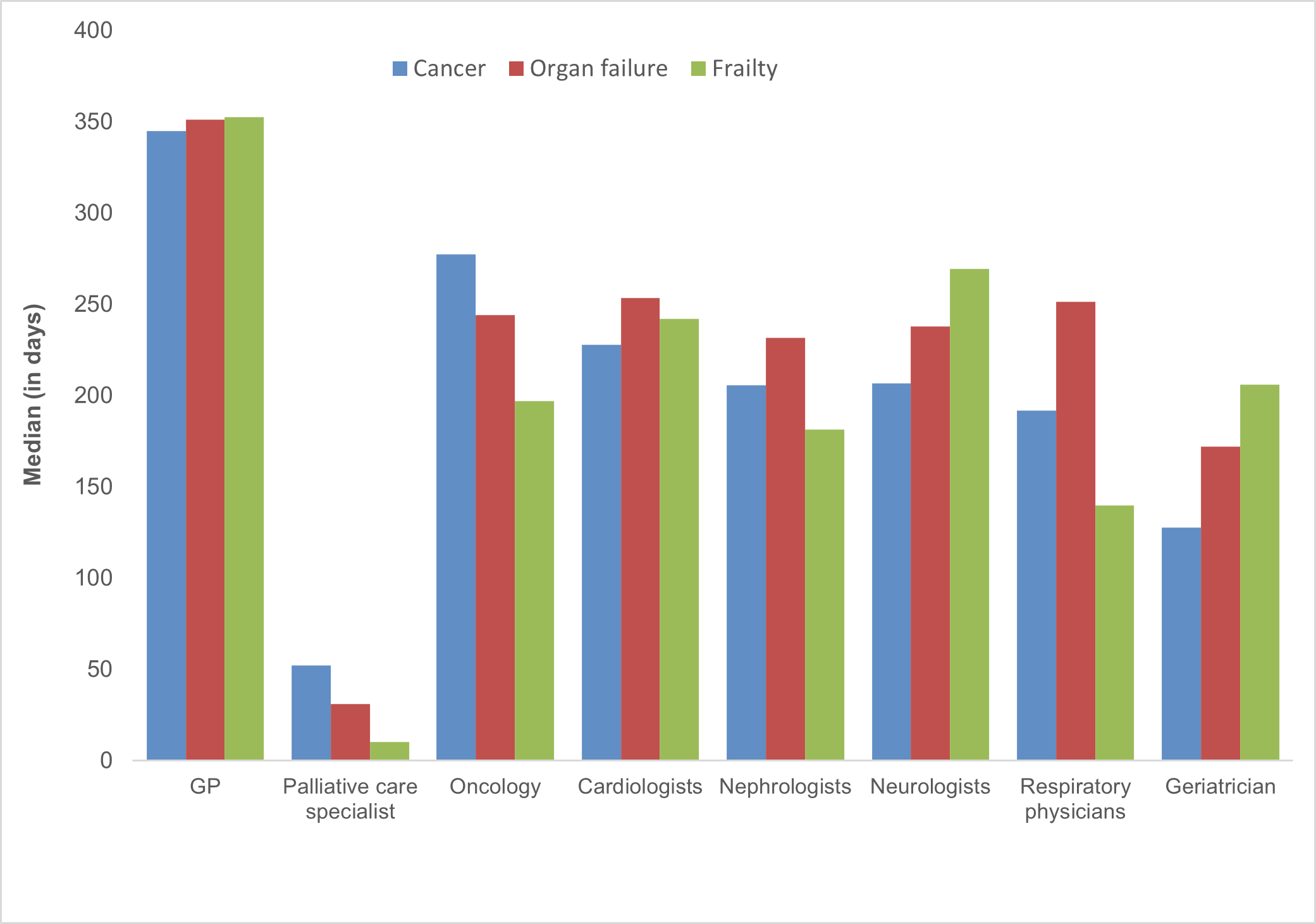
Source: Supplementary Table 6b.