Study populations
This report examines health service use for multiple study populations, as described below and as shown in Figure 2.1.
Predictable deaths population
There were 164,398 deaths between 1 July 2019 and 30 June 2020 (identified from the NDI, based on date of death), of which 93% (or 152,114) were from predictable deaths (not sudden deaths).
Note: Predictable deaths exclude deaths from underlying causes of death during pregnancy, childbirth, or puerperium (ICD code O00–O99); originating during the perinatal period (P00–P96); resulting from injury, poisoning, and certain other external causes (S00–T98) or external causes of morbidity and mortality (V01–Y98).
The analysis was restricted to people aged 40 to <115 years (“40+”) at the time of death and records where sex was missing/indeterminate were excluded. This resulted in 135,617 people (91% of all predictable deaths and 84% of all deaths in 2019-20).
Specialist palliative care population
Of the 135,617 people aged 40+ years who died from predictable deaths in 2019-20, 52,105 people (38%) received specialist palliative care in the last year of life (referred to as the specialist palliative care (SPC) population). The remaining 83,512 people not receiving specialist palliative care are referred to as the non-SPC population.
Population in need of palliative care
From a population-based monitoring and research perspective there is currently no agreed diagnostic definition on who is eligible and should receive palliative care. However, various studies have used epidemiological approaches, based on mortality and hospital admission data, to estimate the size of the population in potential need of palliative care (defined here as those who would potentially benefit from palliative care).
The mortality condition-specific approach in estimating the size of the palliative care population was initially developed by Rosenwax (2005) (see also Rosenwax (2016)) and expanded and refined by Murtagh (2014) which was deemed to be the most appropriate for this project relying on routinely available administrative data (mortality and hospital data), available in NIHSI. Appendix B includes further details on these population-based methods for estimating palliative care need, including an assessment of the appropriateness of various methods.
To create a population in need of palliative care, the predictable deaths population was restricted to only include people who died from specific underlying causes of death that are potentially amenable to receiving palliative care, based on the Murtagh (2014) minimal estimate method (see Appendix Table A3 and Appendix B for further details). The population in need of palliative care captured 109,059 deaths, or 80% of all predictable deaths in 2019-20.
Note that the definition of the population in need of palliative care is based on conditions that most often generate a need for palliative care. However, it cannot be assumed that all people who died from these conditions required specialist palliative care. For example, they may have received appropriate palliative care from other health professionals.
Figure 2.1: Study populations
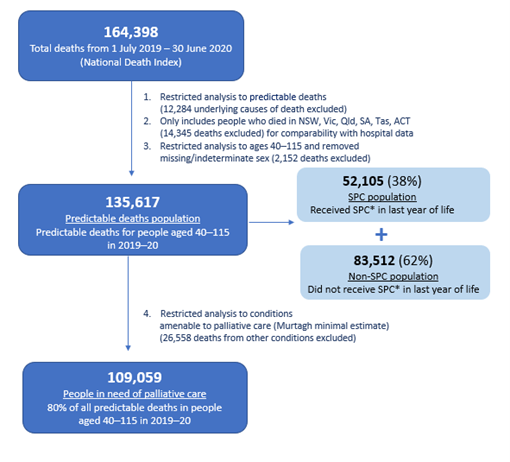
Note: *Specialist palliative care (SPC) services are defined as people admitted to hospital for palliative care (care type or diagnosis of palliative care), attending outpatient hospital clinic services (consultations with palliative medicine physician/specialist), and consultations with palliative medicine specialist/physician (based on MBS claim items).