Antenatal care
Telehealth services
In response to the COVID-19 pandemic, the Australian Government expanded telehealth items to the Medicare Benefits Schedule (MBS) in March 2020, including antenatal care items. These temporary items included antenatal attendances and services provided by video-conference or telephone, which became permanent from 1 January 2022. Note that the MBS items used for analysis in this report may not capture all items that health providers use when providing antenatal care.
Overall, telehealth-integrated antenatal care can be a viable alternative to in-person consultations without compromising pregnancy outcomes (Atkinson et al. 2023; Thirugnanasundralingam et al. 2023). However, uncertainty remains around whether telehealth during the pandemic led to underdiagnosis of maternal conditions such as gestational diabetes and hypertension (Abelman et al. 2023; Thirugnanasundralingam et al. 2023).
In a recent survey of Australian midwives and pregnant women, respondents stated that they positively valued the integration of telehealth services into their maternity care (Kluwgant et al. 2022).
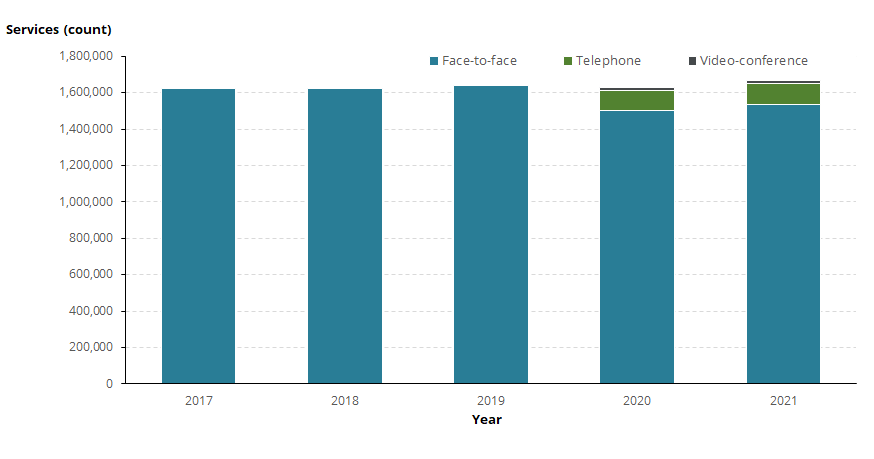
Figure 4 presents MBS data on the types of antenatal care services in Australia.
Figure 4: Number of MBS antenatal care services in Australia, by type of service, 2017 to 2021
Notes:
- Face-to-face (antenatal care) services includes MBS items 16400, 16500, 16590, 16591, 82100, 82105 and 82110.
- Telehealth (antenatal care) services delivered by video-conference includes MBS items 91211, 91212, 91850 and 91853. These items were added to the MBS on 13 March 2020, therefore no data is available prior to this date.
- Telehealth (antenatal care) services delivered by telephone includes MBS items 91218, 91219, 91855 and 91858. These items were added to the MBS on 13 March 2020, therefore no data is available prior to this date.
- State/Territory is determined according to the address (at time of claiming) of the individual to whom the service was rendered.
- The MBS is a billing scheme and the data are subject to provider’s clinical judgment and billing discretion. This means that services may not be billed with 100% accuracy, and they could also be billed outside of the MBS.
- Due to the nature of the MBS, the use of general time-tiered items, and lack of antenatal subspeciality items for some professions, not all services will be clearly represented. For example, currently there are no specific telehealth antenatal items available for Nurse Practitioners to claim. As such, any antenatal services provided by Nurse Practitioners would be claimed under broader telehealth items available.
Source: AIHW analysis of Medicare Benefits Schedule item reports on the Services Australia website on 15 February 2024.
Overall, there were a similar number of antenatal services provided between 2017 and 2020 (ranging from 1.62 million to 1.64 million) and a higher number of services delivered in 2021 (1.67 million).
Between 2017 and 2019, face-to-face delivery was the only type of antenatal care available, with over 1.6 million services provided each year.
In 2020 – after the introduction of MBS telephone and videoconference antenatal care services – face-to-face visits decreased to below 1.5 million visits, or 92% of antenatal care services. Telephone and video-conference accounted for 6.8% and 1.0% of antenatal care services, respectively.
In 2021, face-to-face visits increased to above 1.5 million visits. The type of antenatal care service was mostly face-to-face (92%), followed by telephone (7.1%) and video-conference (0.9%) antenatal care services.
Figure 5 presents data on the type of antenatal care services for states and territories.
Figure 5: Proportion of antenatal care services, by type of service and state or territory of usual residence, 2020 and 2021
Bar chart shows proportion of type of antenatal care delivery between 2020 and 2021.

Line graph shows duration of pregnancy at first antenatal visits by state and territory of birth between 2015 and 2021.

Line graph shows primiparous and multiparous women by number of antenatal visits by state and territory of birth between 2016 and 2021.

Line graph shows primiparous and multiparous women by number of antenatal visits by state and territory of birth between 2015 and 2021.

Map shows proportion of women who had 5 or more antenatal visits by selected geographies and years.
