Chronic respiratory conditions:
Chronic obstructive pulmonary disease
Web article
Last updated:
Citation
AIHW
Australian Institute of Health and Welfare (2024) Chronic obstructive pulmonary disease , AIHW, Australian Government, accessed 30 June 2024.
APA
Australian Institute of Health and Welfare. (2024). Chronic obstructive pulmonary disease . Retrieved from https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd
MLA
Chronic obstructive pulmonary disease . Australian Institute of Health and Welfare, 17 June 2024, https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd
Vancouver
Australian Institute of Health and Welfare. Chronic obstructive pulmonary disease [Internet]. Canberra: Australian Institute of Health and Welfare, 2024 [cited 2024 Jun. 30]. Available from: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd
Harvard
Australian Institute of Health and Welfare (AIHW) 2024, Chronic obstructive pulmonary disease , viewed 30 June 2024, https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd
This article is part of Chronic respiratory conditions
This figure shows that the prevalence of COPD was higher in females aged 55–64 and 65–74 compared with males of the same age.

This figure shows that females with COPD had a higher proportion of non-fatal burden (also known as years lived with disability or YLD) than males with COPD in 2023.

This figure shows that, of people with COPD living in ‘Remote and very remote’ areas, males had higher rates of total burden than females.

This figure shows that $197 million (25%) of COPD expenditure was attributed to the Pharmaceutical Benefits Scheme.

This figure shows that 0.7% of COPD expenditure was attributed to public hospital emergency departments.

This figure shows that the death rate due to COPD (as underlying cause) increased with increasing age and was highest for people aged 85 and over in 2022.

This figure shows that the death rate due to COPD (for underlying cause of death) was highest in 2017 and lowest in 2020.

Variation between population groups
In 2022, after adjusting for age differences, mortality rates for COPD (as the underlying cause) were:
- 1.9 times higher for people living in Remote and very remote areas compared with people living in Major cities (34.8 and 18.8 per 100,000 population, respectively)
- 2.7 times higher for people living in areas of most disadvantage compared with people living in the least disadvantaged areas (31.9 and 11.6 per 100,000 population, respectively).
The same patterns were observed for COPD deaths as an underlying cause or any cause (underlying or associated cause) of death.
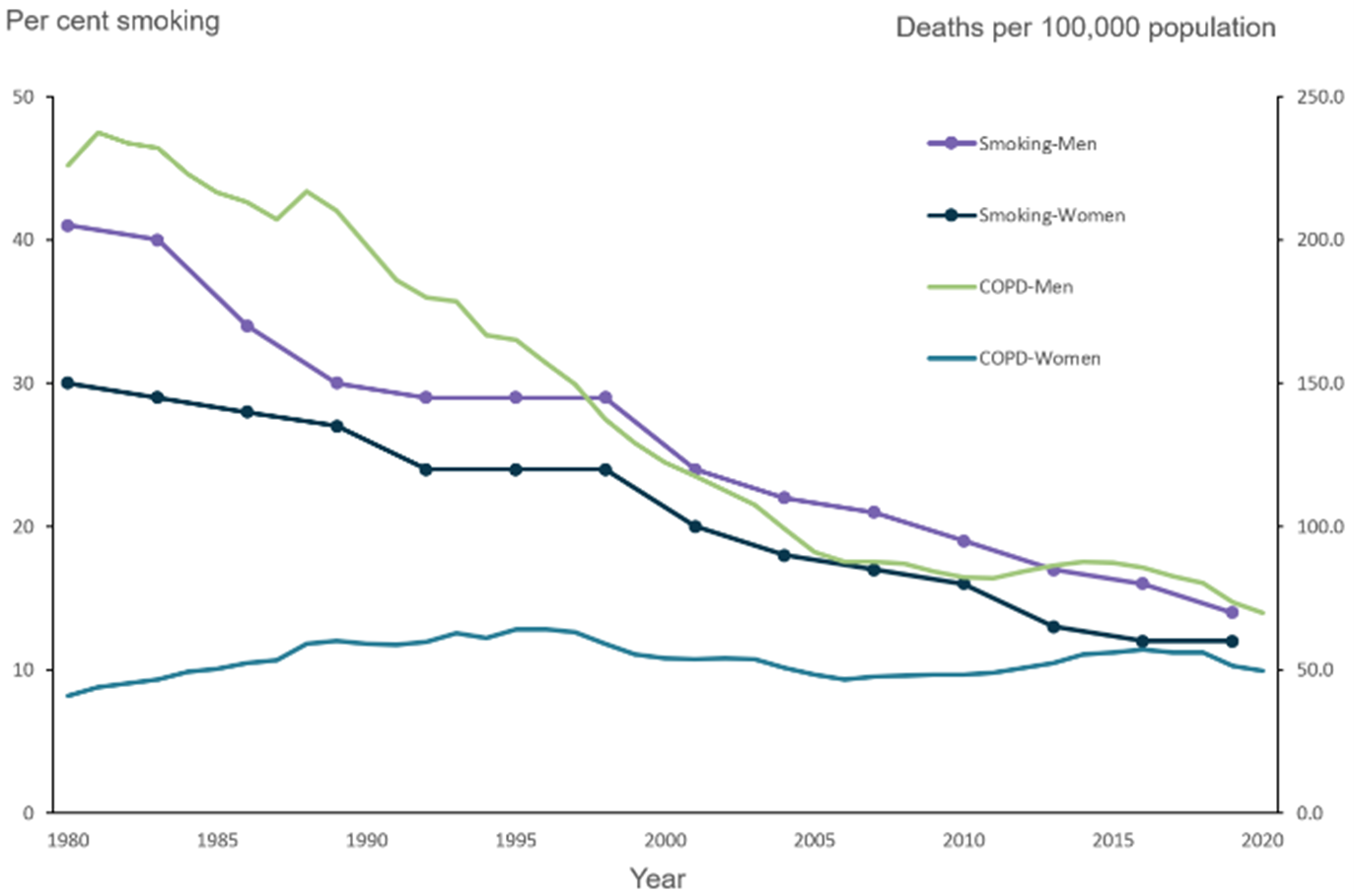
Chronic obstructive pulmonary disease mortality and smoking trends
According to the 2018 Australian Burden of Disease Study, tobacco use contributed to 73% of total disability-adjusted life years (DALY) for COPD. The proportion of DALY attributed to tobacco use was higher among females compared with males (79% and 66%, respectively) (AIHW 2021).
The main risk factor for the development and progression of COPD is smoking, with smokers in the United States being 12 to 13 times more likely to die from COPD than non-smokers (U.S. Department of Health and Human Services 2014).
Improvements in COPD mortality rates tend to follow decreases in smoking rates, with a time-lag in-between due to the long latency period of COPD (smoking early in life is involved in initiating disease processes prior to the disease being diagnosed) (Laniado-Laborin 2009).
In Australia, the smoking rate of adults aged 18 and over decreased from 1980 to 2019 for both men and women, with men having consistently higher smoking rates than women (men: 41% to 14%, women: 30% to 12%) (Figure 8) (Greenhalgh et al. 2023).
For more information on the history of smoking and COPD, see Mortality from asthma and COPD in Australia (AIHW 2014).
Figure 8: Chronic obstructive pulmonary disease death rates of people aged 45 and over, 3-year moving average, and smoking rates, 1980 to 2020
Notes
- COPD deaths are shown as a 3-year moving average. For example, the 2020 data point represents the average of 2019, 2020 and 2021.
- From 1979 to 1996, COPD classified according to ICD-9 codes 490, 491, 492, 496. From 1997 to 2021, COPD classified according to ICD-10 codes J40–J44.
- Smoking refers to people those reporting that they smoke 'daily' or 'at least weekly', and smoking any combination of combustible cigarettes, cigars, pipes or waterpipes. It does not include use of electronic cigarettes/vapes or other personal vaporising devices where users inhale vapour rather than smoke.
- Smoking data were calculated by the Cancer Council of Victoria. Smoking rates for 1980–1992 were sourced from surveys conducted by the Anti-Cancer Council of Victoria. Smoking rates for 1995–2019 were sourced from the National Drug Strategy Household Survey.
- Deaths registered in 2018 and earlier are based on the final version of cause of death data. Deaths registered in 2019 are based on the revised version and deaths registered in 2020 and 2021 are based on the preliminary version. Revised and preliminary versions are subject to further revision by the Australian Bureau of Statistics (ABS).
Source: AIHW analysis of the AIHW National Mortality Database, Scollo and Winstanley 2019 (Chronic Obstructive Pulmonary Disease 2023 Supplementary data table 4.1).
This figure shows that in 2021–22, hospitalisation rates for COPD were lowest for people aged 0–45 for males and females.

This figure shows that the hospitalisation rate for people aged 45 and over followed the same pattern over time for males and females.

This figure shows that hospitalisations rates for acute respiratory infections were highest in August 2017 and lowest in February 2021.

This figure shows that 14% of people living with COPD reported not having any of the other selected chronic conditions.
