Back problems
Page highlights
‘Back problems’ describes a range of conditions related to the bones, joints, connective tissues, muscles and nerves of the back.
Around 4.0 million (16%) people in Australia were estimated to be living with back problems in 2022.
- Back problems were the third leading cause of disease burden overall, accounting for 4.3% of Australia’s total disease burden in 2023.
- In 2020–21, an estimated $3.4 billion was spent on the treatment and management of back problems, representing 2.2% of total health system expenditure and 23% of expenditure for all musculoskeletal conditions.
- Back problems contributed to 1,112 deaths or 4.3 deaths per 100,000 population in 2022 (0.6% of all deaths).
Treatment and management of back problems
In 2021–22, there were 177,000 hospitalisations with a principal diagnosis of back problems (690 hospitalisations per 100,000 population).
Comorbidities of back problems
In 2022, 72% of people with back problems were estimated to be living with one or more other chronic conditions – the top 3 comorbidities were mental and behavioural conditions (43%), arthritis (34%) and asthma (17%).
What are back problems?
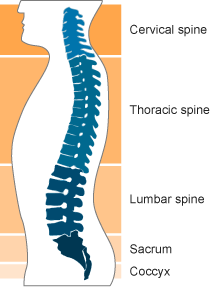
'Back problems’ describes a range of conditions related to the bones, joints, connective tissue, muscles and nerves of the back. These conditions can affect the neck (cervical spine), upper back (thoracic spine) and lower back (lumbar spine) as well as the sacrum and tailbone (coccyx) (Figure 1). Examples of back problems include:
- back or spine pain (such as lower back pain, and sciatica)
- vertebrae and disc disorders (such as narrowing of the spinal canal, and disc degeneration)
- deforming disorders (such as scoliosis).
Figure 1: Lateral view of spine
How common are back problems?
Around 4.0 million (16%) people in Australia were estimated to be living with back problems, according to self-reported data in the 2022 Australian Bureau of Statistics (ABS) National Health Survey (NHS) (ABS 2023). Back problem prevalence increased with increasing age and was similar for males and females.
Note: Unless otherwise stated, crude rates are presented for prevalence in this report and as such, these rates have not been adjusted to account for differences in the age structures of different populations. Care should therefore be taken before making comparisons between populations using these data.
In 2022, people:
- living in Inner and Outer regional areas were more likely to be living with back problems compared with those living in Major cities (17% and 15%, respectively)
- living in areas of most disadvantage (lowest socioeconomic areas) were more likely to be living with back problems compared with people living in the least disadvantaged areas (highest socioeconomic areas) (18% and 13%, respectively)
- with a disability were 4 times as likely to be living with back problems compared with people without a disability (32% and 8%, respectively) (ABS 2023).
After adjusting for different population age structures over time, the prevalence of back problems decreased from 21% in 2001 to 15% in 2022 (Figure 2) (ABS 2023).
Figure 2: Prevalence of back problems, by age and sex, over time (2001 to 2022), by population group, 2022
This figure shows that the prevalence of back problems was highest in males aged 55–74.

This figure shows that both fatal and non-fatal burden were similar for males and females in 2023.

This figure shows the rate of non-fatal burden from back problems was highest for people living in ‘Inner regional’ areas in 2018.

This figure shows that the public hospital admitted patients’ proportion of back problems expenditure was $435 million (12.9%) in 2020-21.

This figure shows that 4.8% of back problem expenditure was attributed to allied health and other services.

This figure shows that between 2012 and 2022, death rates (underlying and/or associated cause) due to back problems were highest in 2022 and lowest in 2013 and 2014.

This figure shows that hospitalisation rates for back problems increased with increasing age up to the 80–84 age group, decreasing thereafter.

This figure shows that between 2015–16 and 2021–22, back problems hospitalisation rates were consistently higher for females compared with males.

This figure shows that 28% of people living with back problems reported not having any of the other selected chronic conditions.
