Mental health
Mental health services provided in emergency departments
About 287,500 mental health-related presentations

to public emergency departments in 2022–23, which was 3% of all presentations
27% had a principal diagnosis of Mental and behavioural disorders due to psychoactive substance use

making this the most frequent diagnosis
59% seen on time

based on triage status compared with 65% across all ED presentations
Infographic containing: 1) Number and rate (per 10,000) of mental health-related emergency department (ED) presentations from 2014–15 to 2022–23; 2) Primary diagnoses in mental health presentations to EDs from 2014–15 to 2022–23; 3) Percentage of mental health-related ED presentations triaged as Urgent, Emergency or Resuscitation during 2022–23 (74%); and 4) Percentage of mental health-related ED presentations classified as seen on time during 2022–23 (59%).
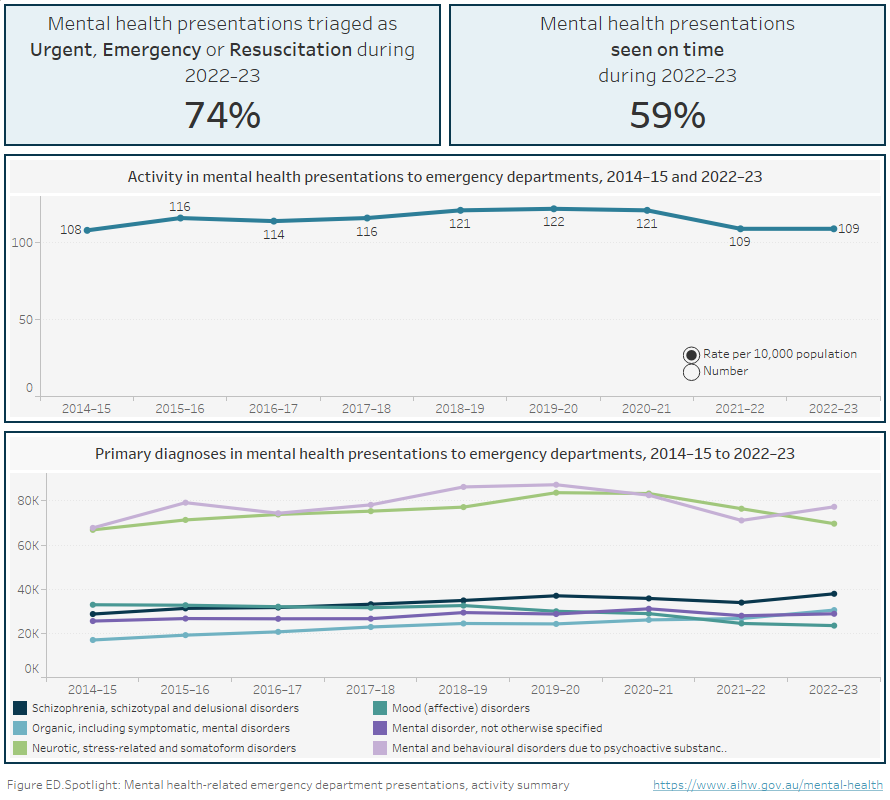
Figure ED.1 Horizontal bar chart showing the rate (per 10,000 population specific) of mental health-related emergency department presentations in public hospitals by patient demographics in 2022–23. Patients 85 years and over had the highest rate of mental health-related ED presentations at 221, followed by 18–24 years (174), 25–34 (150), 35–44 (143), 12–17 (132), 45–54 (125), 75–84 (103), 55–64 (81), 65–74 (58), and 0–11 (13). Males presented at a slightly higher rate than females (111 and 107 respectively). First Nations Australians presented at a higher age-standardised rate than non-Indigenous Australians (491 and 94 respectively). The rate increased with increasing remoteness of remoteness area of usual residence: 97 per 10,000 in Major cities, 114 in Inner regional areas, 126 in Outer regional areas and 239 in Remote and Very remote areas. Mental health-related presentations increased with increasing social disadvantage with 144 presentations per 10,000 for the most disadvantaged quintile (Quintile 1), followed by 125 (Quintile 2), 96 (Quintile 3), 89 (Quintile 4) and 74 for the least disadvantaged quintile (Quintile 5). Refer to Table NED.4.
Figure ED.1.1 Line chart of rate of mental health-related emergency department presentations (per 10,000 population) for age group by sex, 2014–15 to 2022–23. Refer to Table NED.4.
Figure ED.1.2 Line chart of mental health-related emergency department presentations (per 10,000 population) by demographic characteristics, 2014–15 to 2022–23. Refer to Table NED.4.
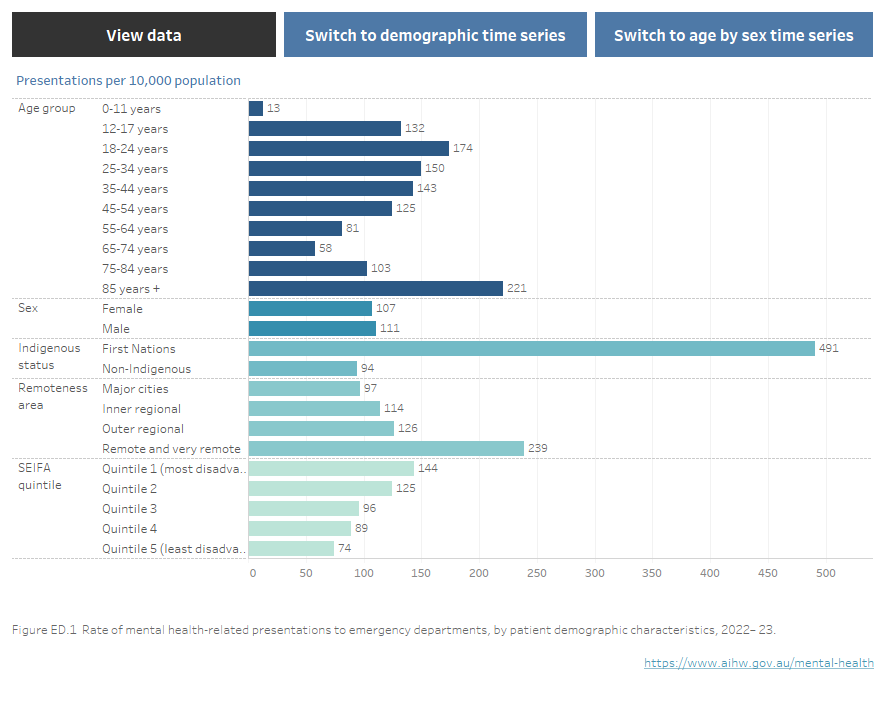
Figure ED.2: Horizontal bar chart showing mental health-related emergency department presentations in public hospitals by principal diagnosis in 2022–23. The majority of presentations were for Mental and behavioural disorders due to psychoactive substance use, making up 27% of presentations, followed by Neurotic, stress-related and somatoform disorders, 24%, Schizophrenia, schizotypal and delusional disorders, 13%; Organic, including symptomatic, mental disorders, 11%; Mental disorder, not otherwise specified 10%; Mood (affective) disorders 8%; Behavioural and emotional disorders with onset usually occurring in childhood and adolescence, 3%; Disorders of adult personality and behaviour, 2%; Behavioural syndromes associated with physiological disturbances and physical factors, 2%; and Disorders of psychological development and Mental retardation (reported as combined categories due to low numbers) >1%.
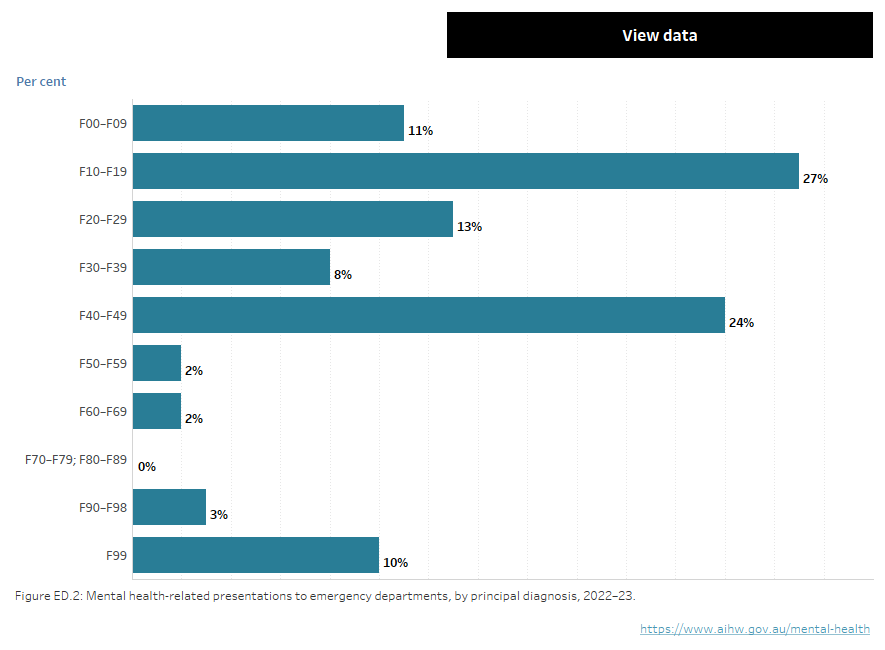
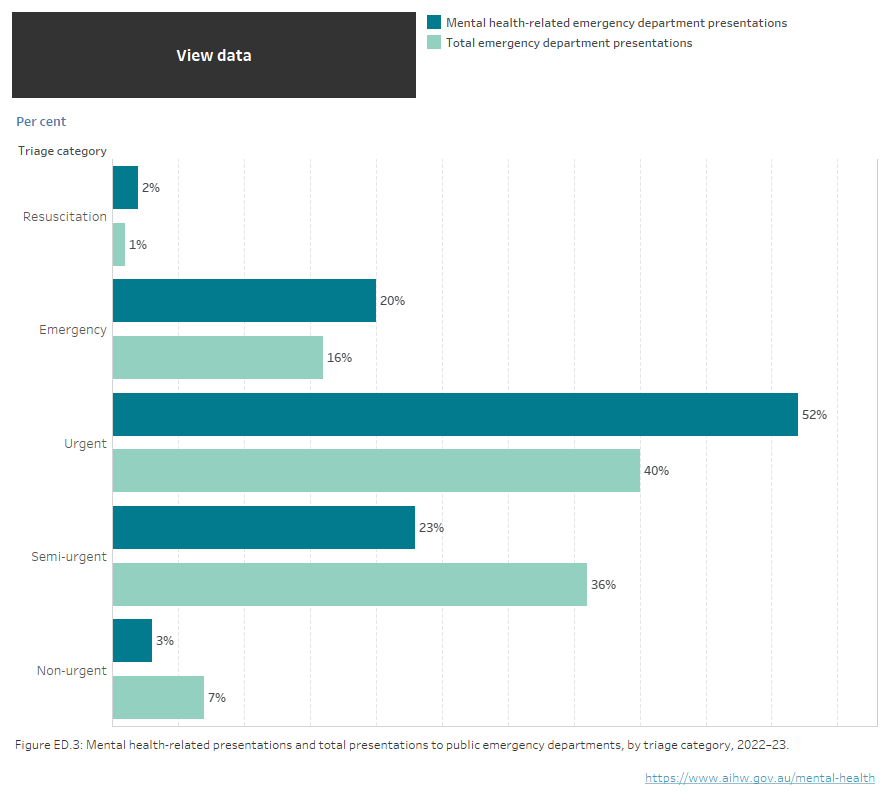
Figure ED.3: horizontal bar chart showing the percentage of mental health-related ED presentations and all ED presentations in public hospitals by triage category. Compared with across all ED presentations, mental health-related ED presentations in 2022–23 had higher proportions of presentations classified as Urgent (52% compared with 40%) Emergency (20% compared with 16%) and Resuscitation (2% compared with 1%), and lower proportions of presentations classed as Semi-urgent (23% compared with 36%) and Non-urgent (3% compared with 7%). Refer to Table NED.1.