Acute rheumatic fever and rheumatic heart disease
Page highlights:
How many Australians have rheumatic heart disease?
- In 2019, there were 5,385 people living with rheumatic heart disease recorded on registers in Queensland, Western Australia, South Australia and the Northern Territory.
- There were 4,600 hospitalisations with a principal diagnosis of acute rheumatic fever or rheumatic heart disease in 2020–21.
- In 2020–21, the rate of hospitalisation for acute rheumatic fever or rheumatic heart disease among Indigenous Australians was 7 times as high as the non-Indigenous rate.
 Acute rheumatic fever or rheumatic heart disease was the underlying cause of 338 deaths in 2019.
Acute rheumatic fever or rheumatic heart disease was the underlying cause of 338 deaths in 2019.
What are acute rheumatic fever and rheumatic heart disease?
Acute rheumatic fever
Acute rheumatic fever (ARF) is an autoimmune response to an infection of the upper respiratory tract by group A streptococcus bacteria. The infection can cause inflammation throughout the body including the heart, brain, skin and joints.
ARF is rare among most Australians, but still has a substantial impact on Aboriginal and Torres Strait Islander communities.
Early detection and treatment can prevent the bacterial infection progressing to ARF. The risk of ARF recurrence is high following an initial episode, and repeated episodes increase the chance of long-term heart valve damage.
Rheumatic heart disease
Rheumatic heart disease (RHD) is permanent damage of the heart muscle or heart valves as a result of ARF. RHD reduces the ability of the heart to pump blood effectively around the body, leading to symptoms such as shortness of breath after physical activity, fatigue and weakness. Severe forms can result in serious incapacity or death.
Symptoms of RHD can also occur with other heart conditions, making a diagnosis more difficult. Signs of damage detected by echocardiography and a history of ARF are both important clinical indicators for RHD diagnosis.
Risk factors and prevention of acute rheumatic fever and rheumatic heart disease
ARF and RHD are closely associated with social and environmental factors such as poverty, overcrowding, and reduced access to health care.
Secondary prevention of the progression from ARF to RHD relies on correct diagnosis, to enable commencement of regular antibiotic preventive medication. Guidelines recommend admission to hospital for clinical investigation and confirmation of the diagnosis of ARF (RHD Australia 2020).
Effective prevention, diagnosis and treatment remain a challenge in remote Indigenous communities. Under the Rheumatic Fever Strategy (RFS), the Australian Government provides funding to support RHD control programs in Queensland, Western Australia, South Australia and the Northern Territory.
Notifications of acute rheumatic fever
There were 2,244 notifications of ARF were recorded in Queensland, Western Australia, South Australia and the Northern Territory in 2015–2019 (4.7 per 100,000 population) (AIHW 2021). Of these:
- 95% (2,128 ARF notifications) were recorded among Indigenous Australians – a rate of 96 per 100,000 population over 2015–2019
- ARF was more common among Indigenous females than males, and rates were highest among Indigenous people aged 5–14 (1,029 notifications, 208 per 100,000)
- the number and rate of notifications has increased – from 342 (3.7 per 100,000) in 2015 to 477 (5.0 per 100,000) in 2019.
How many Australians have rheumatic heart disease?
As at 31 December 2019, there were 5,385 (56 per 100,000 population) people living with RHD recorded on registers in Queensland, Western Australia, South Australia and the Northern Territory (AIHW 2021).
Of these:
- 81% were Indigenous Australians (4,337 diagnoses, 955 per 100,000 population)
- 39% were aged under 25 (1,558 diagnoses)
- 66% were female (3,561 diagnoses)
- Northern Territory had the highest prevalence (2,308 diagnoses, 938 per 100,000).
Of those RHD diagnoses with severity status recorded, 41% had mild disease (2,206 diagnoses), while 28% had severe disease (1,532).
Older people were more likely to have severe RHD, with 42% aged 45 or over having severe disease (777 diagnoses), compared to 16% of those aged 15–24 (173 diagnoses).
New rheumatic heart disease diagnoses
In 2015–2019, there were 1,776 new RHD diagnoses in Queensland, South Australia, Western Australia and the Northern Territory (3.7 per 100,000 population).
Of these, 75% (1,325) were Indigenous Australians (60 per 100,000 population).
For the 4 jurisdictions combined, RHD diagnosis rates between 2015 and 2019 have remained relatively stable, at around 3–4 diagnoses per 100,000 population annually (Figure 1).
During this period, diagnosis rates varied by state and territory, but in general:
- South Australia had less than 1 diagnosis per 100,000 population
- Western Australia and Queensland had 2–5 diagnoses per 100,000
- Northern Territory had 40–60 diagnoses per 100,000.
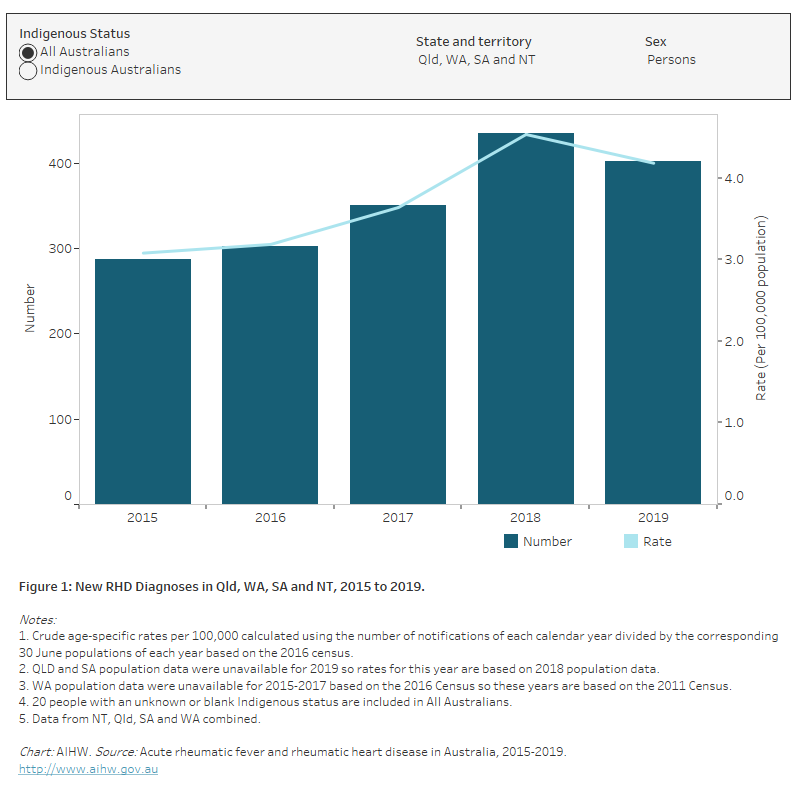
Figure 1: New RHD diagnoses in Qld, WA, SA and NT, 2015 to 2019
The bar chart shows the number and rate of new rheumatic heart disease diagnoses in Queensland, Western Australia, South Australia and the Northern Territory in 2015-2019. Among all Australians in these four states and territories combined, there was an increase in the age-standardised rate of new rheumatic heart disease diagnoses between 2015 and 2018 (3.1 to 4.5 per 100,000 population). The age-standardised rate of new rheumatic heart disease diagnoses was consistently higher among Indigenous Australians compared to the total Australian population.
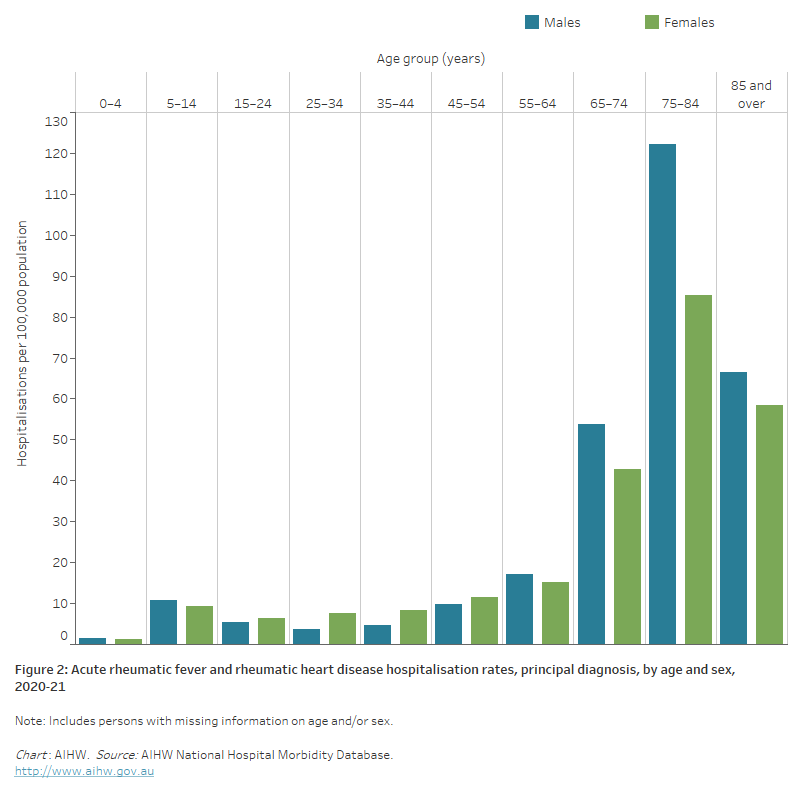
The bar chart shows in 2020–21 acute rheumatic fever and rheumatic heart disease hospitalisation rates were highest among males and females aged 75–84 years with 122 and 85 hospitalisations per 100,000 population, respectively.
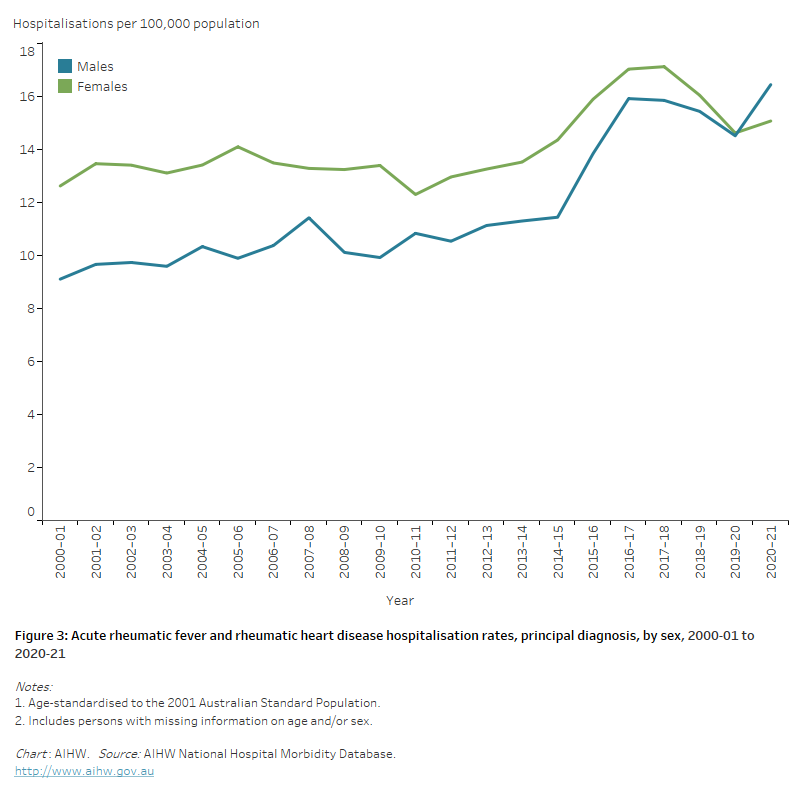
The line chart shows the overall increase in age-standardised acute rheumatic fever and rheumatic heart disease hospitalisation rates between 2000–01 and 2020–21 from 9.1 to 16.5 and 12.6 to 15.1 per 100,000 population for males and females, respectively.
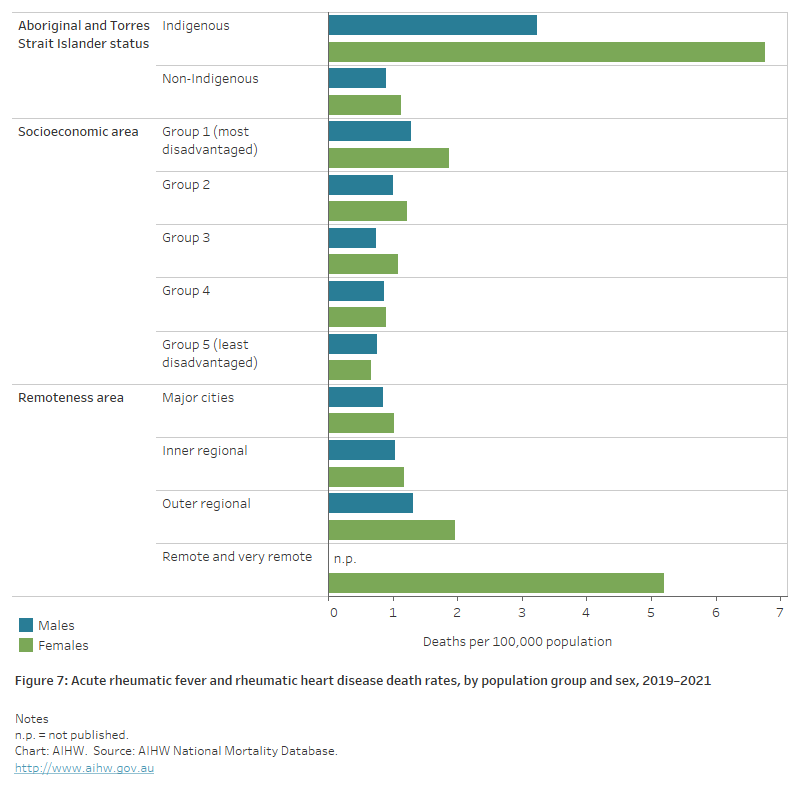
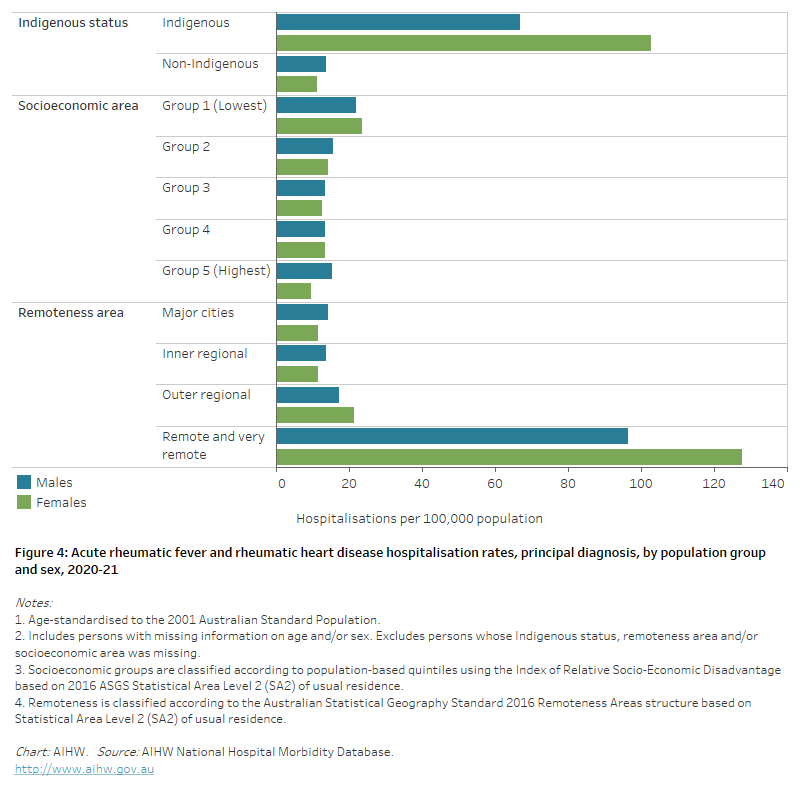
The horizontal bar chart shows in 2020–21 age-standardised acute rheumatic fever and rheumatic heart disease hospitalisation rates were higher among Indigenous Australians, people living in the lowest socioeconomic areas and people living in Remote and very remote areas.
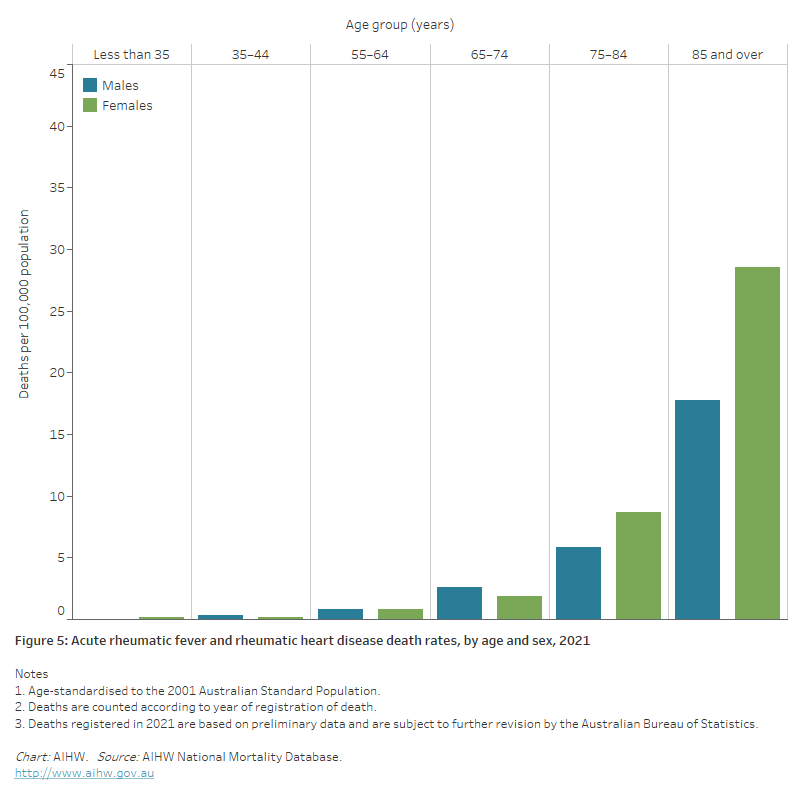
The bar chart shows in 2021 acute rheumatic fever and rheumatic heart disease death rates were highest among males and females aged 85 and over, at 18 and 29 per 100,000 population, respectively.
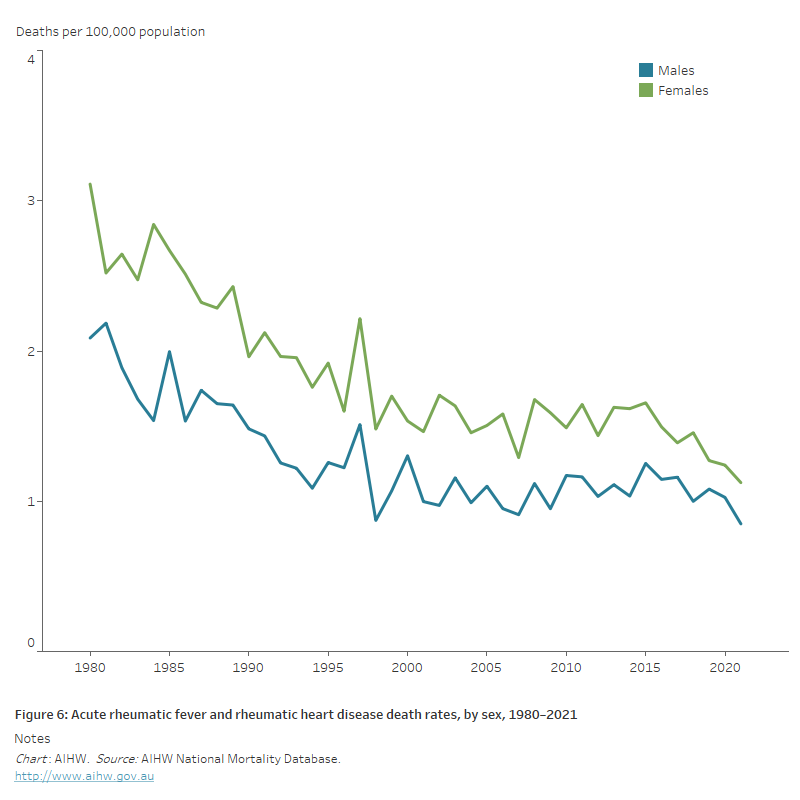
The line chart shows the decline in age-standardised acute rheumatic fever and rheumatic heart disease death rates between 1980 and 2021 from 2.1 to 0.8 and 3.1 to 1.1 for males and females, respectively.
The horizontal bar chart shows in 2019–2021 age-standardised acute rheumatic fever and rheumatic heart disease death rates were higher among Indigenous Australians, people living in the lowest socioeconomic areas and people living in Remote and very remote areas.