Page highlights
In 2020–21, 1.6 million (14%) of hospitalisations in Australia were for dialysis.
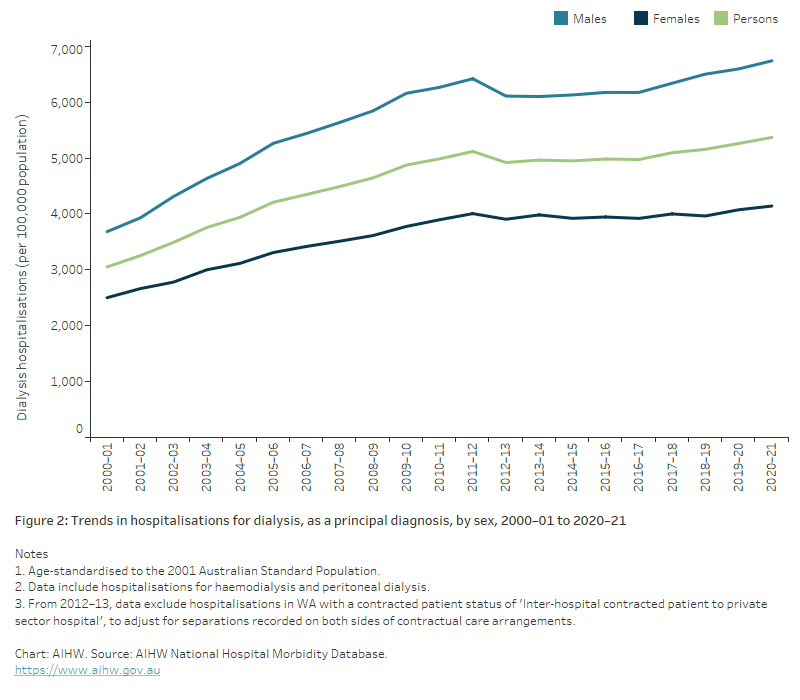
The number of hospitalisations for dialysis nearly tripled between 2000–01 and 2020–21, from 582,000 to 1.6 million.
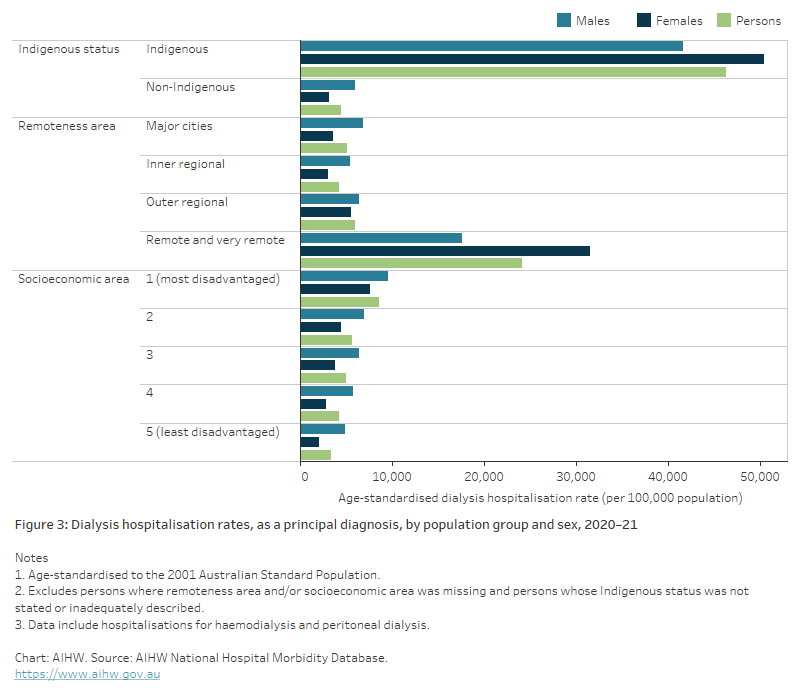
In 2020–21, there were 264,000 hospitalisations for dialysis (as the principal diagnosis) among Aboriginal and Torres Strait Islander people, 30,300 per 100,000 population.
Dialysis is the most common reason for hospitalisation in Australia, accounting for 14% of all hospitalisations in 2020–21 (1.6 million hospitalisations). Although the majority of people admitted to hospital for dialysis receive haemodialysis, a small number receive peritoneal dialysis. Data on this web page includes hospitalisations for both types of dialysis.
Hospitalisation data count the number of dialysis episodes rather than the number of people who receive dialysis. Most people undergoing dialysis attend 3 sessions per week (ANZDATA 2021).
For more information about people receiving dialysis, see Dialysis.
What is dialysis?
Dialysis is an artificial way to remove waste and excess water from the blood, and regulate safe levels of circulating agents (such as potassium, calcium and phosphorous) in the body, a function usually performed by the kidneys. It is most often provided to treat chronic kidney failure, but is sometimes needed in cases of acute kidney failure, where the kidneys have been temporarily damaged due to illness or injury.
There are 2 types of dialysis: peritoneal dialysis and haemodialysis.
Peritoneal dialysis is an internal filtration process requiring the placement of a catheter (a thin, flexible plastic tube) into the abdomen, which remains in place as long as dialysis is required. Peritoneal dialysis uses the peritoneal membrane inside the abdominal cavity to filter the blood inside the body.
The process involves filling the abdomen with a sterile dialysis solution, called dialysate. Over 4–8 hours, waste is drawn out of the blood through the peritoneal membrane and into the dialysate. The used solution is then drained out of the body and replaced with a new solution. This process is called an exchange and takes around 30–45 minutes.
Between exchanges, the person is free to continue their usual activities. Peritoneal dialysis can be performed either by the person 3 or 4 times during the day (continuous ambulatory peritoneal dialysis) or automatically by a machine at night for about 8–10 hours while the person sleeps (automated peritoneal dialysis).
As the necessary equipment is portable, peritoneal dialysis can be performed almost anywhere. Individuals do not need to be in a hospital or clinic and can usually manage the procedure without assistance.
Haemodialysis is an external filtration process where the blood is diverted from the body to a machine which removes waste and excess fluid. It involves an initial procedure to join an artery and vein together with either a fistula or graft, that serves as the access point to the dialysis machine (dialyser). Once this access point is ready, haemodialysis sessions take place for an average of 4 to 5 hours 3 times per week (ANZDATA 2021). Once the blood has been filtered by the dialyser, it is returned to the body through the access point.
Haemodialysis can be done at home or in specialised dialysis centres located either in hospitals or satellite units. The process involves specialised plumbing installation for the dialyser and the person requires assistance to be connected to the machine. If performed at home, the procedure may be done more frequently for shorter periods or overnight.
Sources: KHA 2016a, 2016b.
Variation by age and sex
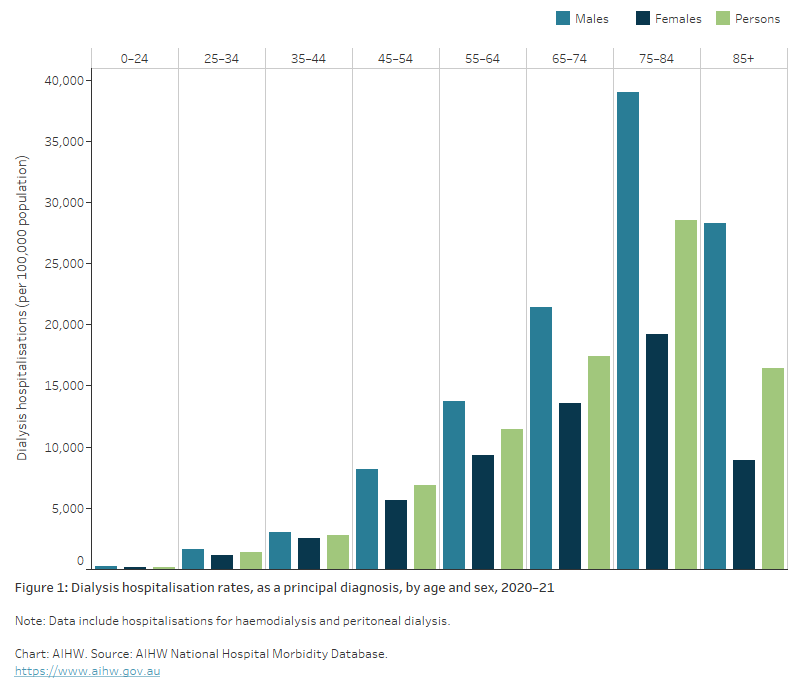
In 2020–21, hospitalisation rates for dialysis as the principal diagnosis:
- were 1.6 times higher in males than in females. Age-specific rates for males were higher than those for females across all age groups
- increased with age up to ages 75–84, with 76% of hospitalisations occurring in people aged 55 and over. Dialysis hospitalisation rates for males and females were highest among those aged 75–84 (39,000 and 19,200 per 100,000 population, respectively) (Figure 1).