Page highlights:
- In 2021, chronic kidney disease contributed to around 20,000 deaths in Australia – 12% of all deaths.
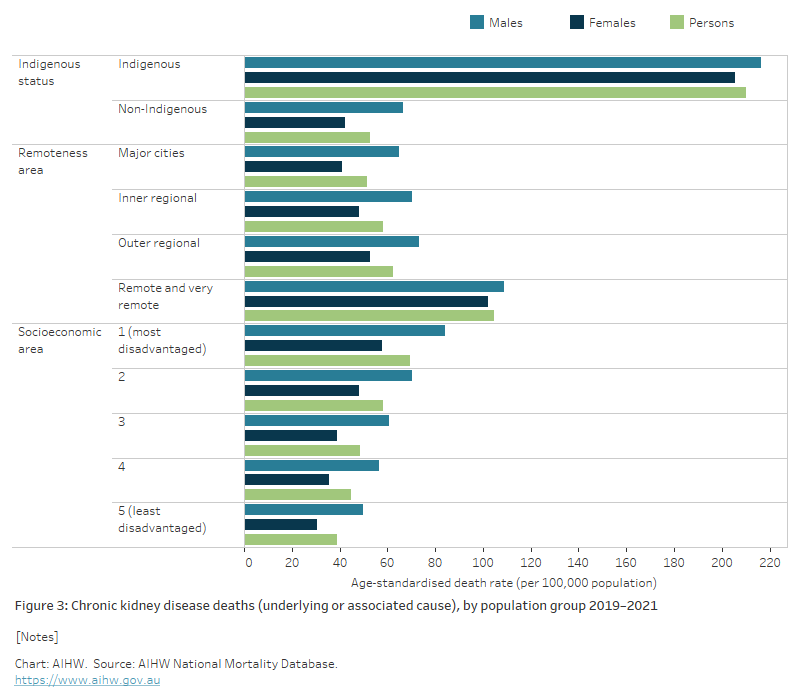
- In 2021, Aboriginal and Torres Strait Islander Australians were 4 times as likely to die from chronic kidney disease as non‑Indigenous Australians.
Chronic kidney disease (CKD) may be listed as the underlying cause of death – or, more commonly, as an associated cause – on a death certificate where another condition is listed as the underlying cause.
In 2021, chronic kidney disease contributed to around 20,000 deaths in Australia – 12% of all deaths.
Of these, CKD was listed as an underlying cause of death in around 4,600 cases (23% of all CKD deaths). It was recorded as an associated cause in a further 15,400 deaths (around 77% of CKD deaths). Deaths with CKD as an underlying or associated cause accounted for 12% of all deaths in Australia in 2021.
Linked data from the Australia and New Zealand Dialysis and Transplant (ANZDATA) Registry and National Death Index has shown that CKD, particularly kidney failure, is often an under-reported cause of death (AIHW 2016).
Diseases commonly listed as underlying causes of death where chronic kidney disease is an associated cause
In cases where CKD was an associated cause of death, the most common groups of underlying causes were:
- diseases of the circulatory system (33%)
- cancers (20%)
- endocrine, nutritional and metabolic diseases (9.4%)
- diseases of the respiratory system (8.0%).
More specifically, the most common underlying causes of death, by 3-digit International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) code, were:
- chronic ischaemic heart disease (10.8%)
- acute myocardial infarction (4.4%)
- heart failure (4.2%)
- other chronic obstructive pulmonary disease (4.1%).
- type 2 diabetes mellitus (4.0%)
- unspecified dementia (4.0%)
In about a third of cases where CKD was listed as an associated cause of death, the underlying cause was a disease of the circulatory system. This reflects the common comorbidity of CKD and cardiovascular diseases (see Comorbidity of chronic kidney disease for more information).
Epidemiological data also suggest that individuals with CKD are at increased risk of experiencing cognitive impairment and of developing dementia (Bugnicourt et al. 2013). This may explain why CKD is commonly listed as an associated cause of death in deaths due to unspecified dementia.
In cases where CKD was the underlying cause of death, the most common groups of associated causes included:
- diseases of the circulatory system (41%) – such as heart failure (10%), primary hypertension (8.3%) and chronic ischaemic heart disease (5.2%)
- endocrine, nutritional and metabolic diseases (14%) – such as type 2 and unspecified diabetes mellitus (5.7% and 3.9%, respectively)
- diseases of the respiratory system (8.0%) – such as pneumonia, organism unspecified (1.9%) and other chronic obstructive pulmonary disease (1.8%)
- diseases of the genitourinary system (6.8%) – such as acute kidney failure with tubular necrosis (5.2%).
Trends over time
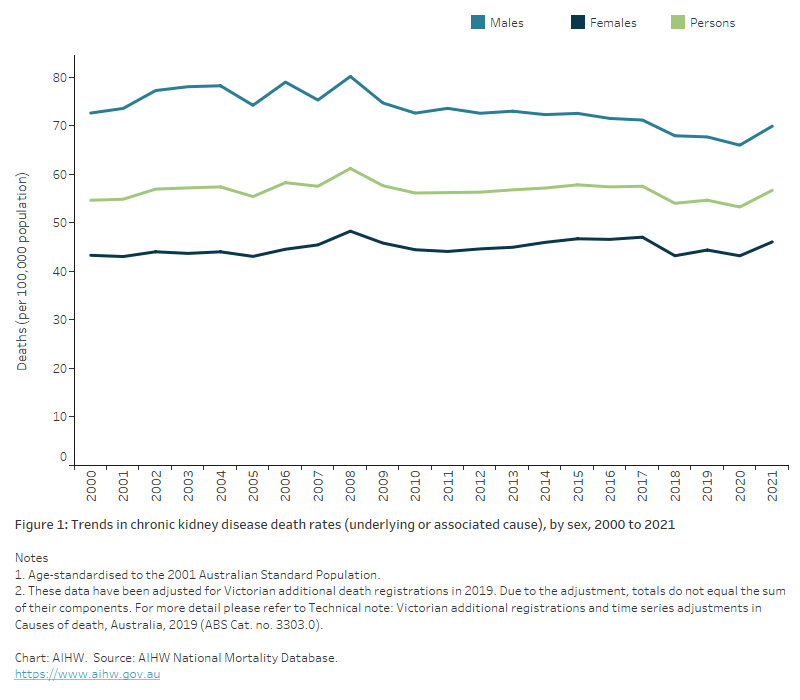
The number of deaths with CKD as an underlying or associated cause rose by 97% between 2000 and 2021 (10,200 and 20,000 deaths). After accounting for changes in the age structure of the population over this time, the rate of CKD deaths remained relatively stable between 2000 and 2021.
Between 2000 and 2021:
- the death rates for males ranged between 66 and 80 deaths per 100,000 population, after adjusting for age (Figure 1)
- the death rate for females was consistently lower than for males, ranging between 43 and 48 deaths per 100,000 population, after adjusting for age (Figure 1).