Variation between population groups
In 2018, the burden from CKD for people living in:
- the lowest socioeconomic areas was 2.2 times as high as for people living in the highest socioeconomic areas (AIHW 2021a)
- Remote and very remote areas was 3.1 times as high as for people living in Major cities.
Trends over time
- The rate of burden from CKD was similar in 2003 and 2023 – age-standardised rates of 1.7 and 1.8 DALY per 1,000 population, respectively (AIHW 2023).
- The 49% increase in DALY from CKD between 2003 and 2018 (+16,200 DALY) was estimated to be driven by population growth (29% or 9,600 DALY) and population ageing (20% or 6,500 DALY) (AIHW 2021a).
First Nations people
Burden of disease estimates for First Nations people for 2018 (AIHW 2022a,b) show that:
- CKD accounted for 2.5% (6,100 DALY) of total burden in First Nations people in 2018 (2.0% males, 3.1% females)
- 73% of the burden from CKD among First Nations people was fatal, and 27% was non-fatal
- the burden from CKD was greater in females (58%, 3,500 DALY) than in males (42%, 2,600 DALY)
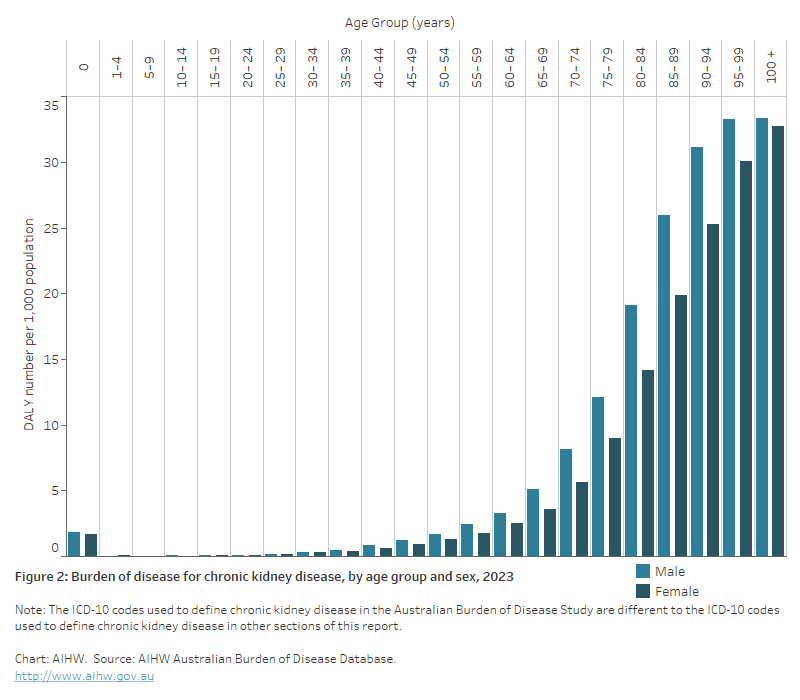
- the burden from CKD rose rapidly in First Nations people from age 40–44, peaking at ages 50–54. Overall, over 80% of the burden from CKD (4,900 DALY) occurred in people aged 40–74
- the rate of burden from CKD was 7.8 times as high for First Nations people as for non-Indigenous Australians
- CKD was responsible for 4.0% of the total male health gap and 6.5% of the total female health gap between First Nations and non-Indigenous Australians.
Contribution of risk factors
A portion of burden of disease is preventable, being due to modifiable health risk factors. The Australian Burden of Disease Study 2018 estimated the disease burden that can be attributed to these modifiable risk factors (AIHW 2021b).
This study provides estimates for burden due to impaired kidney function as a risk factor for other diseases, including coronary heart disease, dementia, stroke, gout and peripheral vascular disease. In 2018, 1.9% of the total disease burden in Australia was due to impaired kidney function (including CKD). Note that the study considers that impaired kidney function was responsible for the entire burden of CKD.
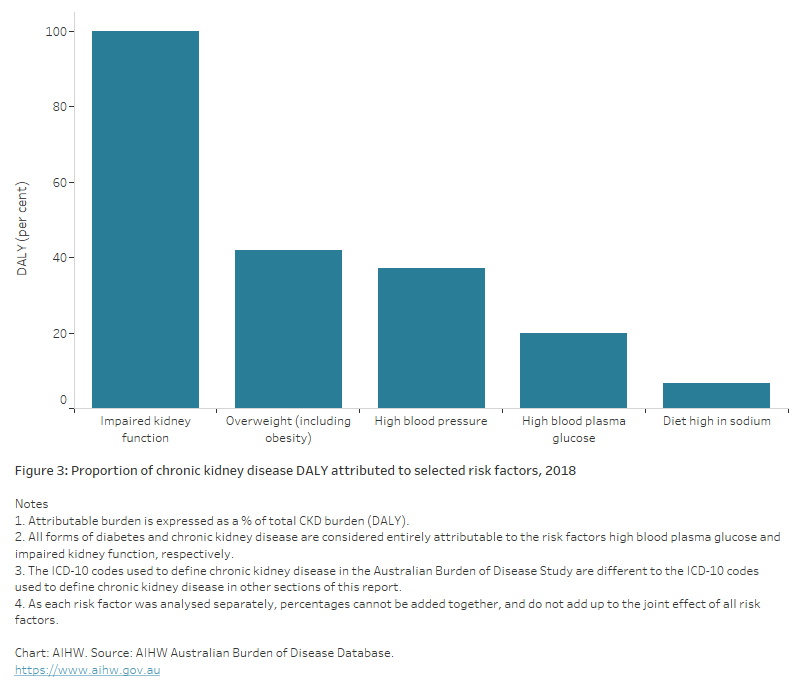
Of the total burden of CKD in Australia in 2018, 100% was attributable to all risk factors combined of those estimated in the study, including impaired kidney function.
The leading risk factors contributing to the total CKD burden in 2018 include impaired kidney function (100% male and female), overweight/obesity (43% male, 40% female), high blood pressure (38% male, 36% female), high blood plasma glucose (20% male and female), and a diet high in sodium (8% male, 5% female) (Figure 3).
Note that as each risk factor was analysed separately, percentages cannot be added together, and do not add up to the joint effect of all risk factors.