What are determinants of health?
Web article
Release Date:
Section: Determinants of health
Citation
AIHW
Australian Institute of Health and Welfare (2024) What are determinants of health?, AIHW, Australian Government, accessed 02 July 2024.
APA
Australian Institute of Health and Welfare. (2024). What are determinants of health?. Retrieved from https://www.aihw.gov.au/reports/australias-health/what-are-determinants-of-health
MLA
What are determinants of health?. Australian Institute of Health and Welfare, 02 July 2024, https://www.aihw.gov.au/reports/australias-health/what-are-determinants-of-health
Vancouver
Australian Institute of Health and Welfare. What are determinants of health? [Internet]. Canberra: Australian Institute of Health and Welfare, 2024 [cited 2024 Jul. 2]. Available from: https://www.aihw.gov.au/reports/australias-health/what-are-determinants-of-health
Harvard
Australian Institute of Health and Welfare (AIHW) 2024, What are determinants of health?, viewed 2 July 2024, https://www.aihw.gov.au/reports/australias-health/what-are-determinants-of-health

There are many factors or ‘determinants’ that influence health, most of them non-medical. Importantly, there is a close relationship between people's health and the circumstances in which they grow, live, work, play and age (Commission on Social Determinants of Health 2008). These in turn influence various health behaviours and other determinants (see glossary).
Health determinants may be risk or protective factors, and they interact to influence the health of individuals and communities. These determinants have a considerable impact on health – often a larger impact than the health care individuals may receive (WHO 2017). Individuals have limited control over many determinants as they are shaped outside their area of influence.
A determinant of health impacts on health and wellbeing by increasing or decreasing the risk of disease or injury occurring. However, people can develop diseases without these risk factors. Also, if someone develops a disease when they do have these risk factors, it does not mean the risk factor caused the disease.
Health determinants include general socioeconomic, cultural and environmental conditions; living and working conditions; social and community networks; and individual behavioural and biological factors. The model in Figure 1 shows how these determinants interact and impact health and wellbeing (Dahlgren and Whitehead 2021).
Figure 1: Model showing layers of health determinants
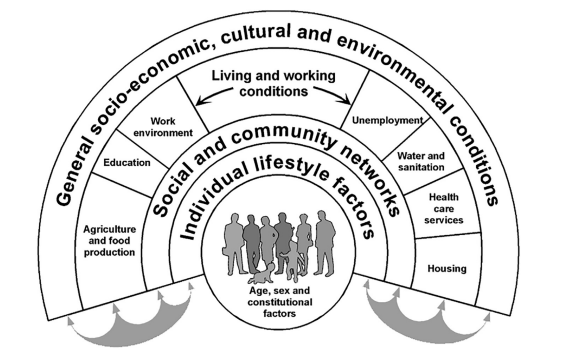
Source: Dahlgren and Whitehead 2021
Understanding health determinants and their relationships
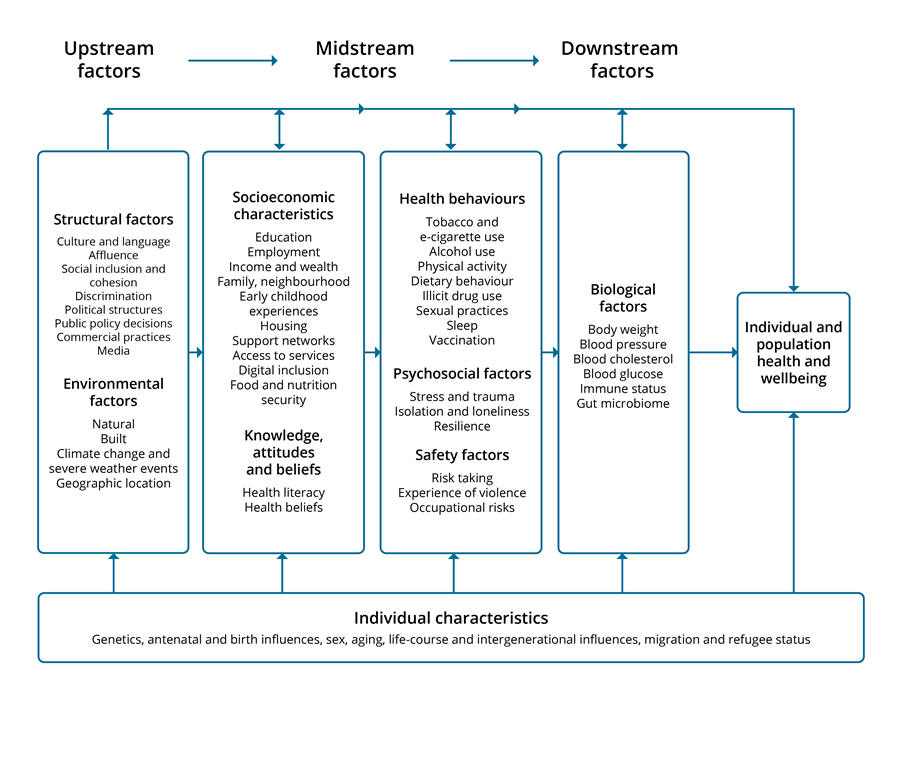
Figure 2 is the AIHW's framework for determinants of health. It shows important non-medical determinants that affect the health and wellbeing of individuals, population groups and the Australian population.
In the framework, determinants that can be modified are divided into 4 main groups (large boxes) and ordered from 'upstream' to ‘downstream’, reflecting the relationships shown in Figure 1. Downstream factors have the most direct impact on health and wellbeing. These downstream factors are influenced by midstream factors, which are in turn influenced by upstream factors. Individuals have more control over downstream than upstream factors like structural and environmental factors. This sequence is known as the causal chain and shows the path through which determinants such as the built environment or public policy can influence health and wellbeing. Determinants within each box often interact with, and are closely related to, each other. While the causal chain largely flows from the upstream to downstream factors, the relationships are complex and there are also influences in the other direction.
Figure 2 also identifies factors that are not generally modifiable (see glossary) once a person has been born. These factors include antenatal and birth influences (including preterm birth and low birthweight), age, sex and intergenerational effects (bottom box). The associations between these and other determinants are important to understand as this will assist with prevention to support better health outcomes.
Figure 2: Framework for determinants of health
The pathways between these determinants and subsequent health outcomes are complex and inter-related. For example, upstream socioeconomic determinants affect many others further downstream, including health behaviours and biological factors. There is also evidence of more direct relationships between socioeconomic determinants and biological factors, such as inflammation (Berger et al. 2019; Hamilton and Steptoe 2023). Health determinants can have different impacts at various life stages, can accumulate over the life course and across generations (Department of Health 2021; van Zwieten 2024). Further, many determinants influence more than one health outcome. This means that improving determinants further upstream (at the system level) is likely to be more effective as it can reduce the risk of poor health outcomes occurring within the population.
Evolution of the framework for health determinants
A framework for health determinants has been included in previous editions of Australia’s health (for example, AIHW 2020, 2010, 2004). The framework has changed over time as research increases our understanding. The current version has been updated to reflect the National Preventive Health Strategy 2021–2030, and now includes commercial practices (see Commercial determinants of health below), discrimination, climate change, digital inclusion, e-cigarette use, isolation and loneliness, resilience, and the gut microbiome. Some previously included determinants have become more prominent in recent times, such as indoor air quality (part of the built environment) and its importance in reducing the risk from communicable diseases including COVID-19, and exposure to pollutants and allergens (Furlow 2023; Braggion et al. 2024). A specific framework for Aboriginal and Torres Strait Islander people has also been developed and used for reporting since 2006 (AIHW 2020), and is consistent with the version in Figure 2, even if not all factors are listed (for example, connection to Country is not stated, but is included under culture and language).
Health determinants impact health and health equity
The focus of Figure 2 is on how health determinants impact on individual and population health and wellbeing. While this includes the important area of socioeconomic determinants, an important additional consideration is how the health determinants affect health inequalities and inequities. Health inequalities are differences in health between groups and health inequities are differences that are avoidable and unfair (see glossary for more information on these concepts).
Understanding how determinants affect health inequalities
In all countries, regardless of national income levels, health and illness follow a social gradient: the lower an individual’s socioeconomic position, the higher their risk of poor health (WHO 2022).
To understand why this is, Diderichsen et al. (2001) developed a conceptual model of the relationship between health determinants and health inequalities (adapted in Figure 3). It relates health inequalities to unequal distribution (differentials) of determinants.
The distribution of power and resources that accompanies the socioeconomic gradient in a society is due to a range of social and structural determinants. Differences in power and resources can cause differentials in determinants. For instance, less power and resources can increase a person’s exposure to health risks, mean they are more vulnerable to disease and injury, and increase the social and economic consequences they may suffer because of ill health (Diderichsen et al 2001; van Zwieten et al. 2024). The model also demonstrates that this relationship is compounding, with the social and economic consequences of ill health affecting upstream determinants that further reduce an individual’s access to power and resources.
Figure 3: How differences in health determinants contribute to health
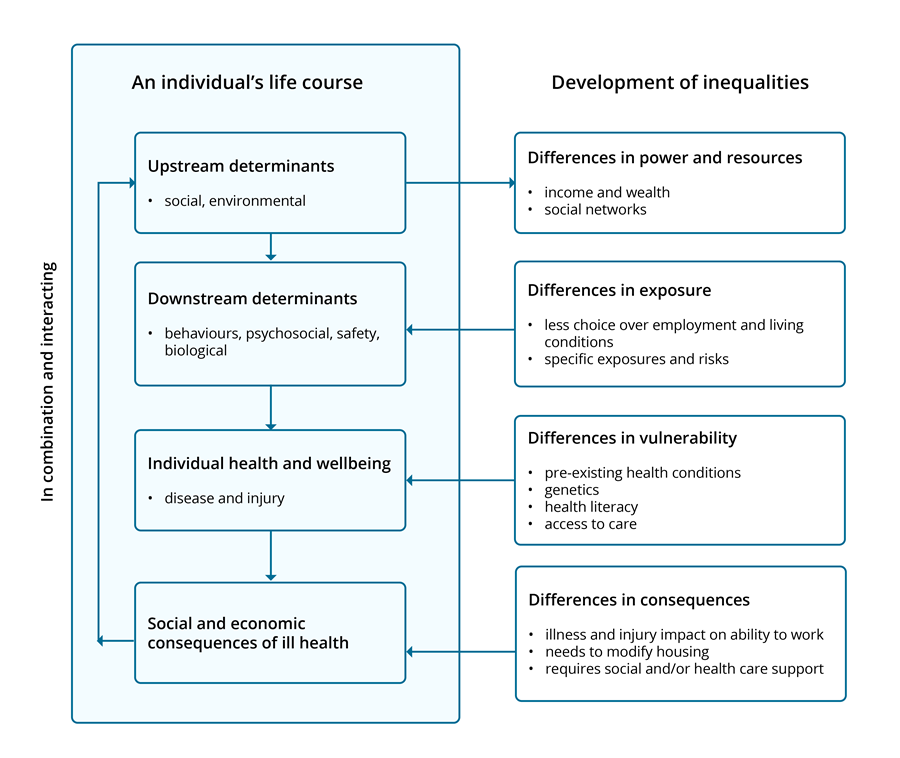
Source: Adapted from Diderichsen, Evans and Whitehead (2001)
Why we need to understand and monitor health determinants
Understanding how health determinants impact health and health equity is important to guide:
- which issues to monitor, with data and information, for the Australian population
- where there is potential for prevention activities which can improve outcomes and reduce costs.
It is important to monitor the prevalence of the determinants, particular groups impacted and whether there are changes over time. This can inform specific policy actions for the whole population or for specific population groups.
Addressing health determinants through prevention
Health prevention is an action to keep people healthy and well, and to prevent or avoid the risk of poor health, illness, injury and early death (The Australian Prevention Partnership Centre n.d.). It aims to increase the likelihood that people will stay healthy for as long as possible. As well as reducing the likelihood that a disease or disorder will affect an individual, it also aims to interrupt or slow the progress of the disorder and reduce associated disability (WHO Global Forum on Chronic Disease Prevention and Control 2004). This is sometimes referred to as secondary and tertiary prevention (Last 2001).
Prevention activities can either be aimed at individuals or small groups (such as quit smoking programs, health advice from general practitioners and preventive treatment such as blood pressure medication), at the community level (for example walking groups) or provided for the whole population (such as advertising campaigns, school-based interventions, taxes, regulations) (AIHW 2009). The most effective prevention programs often have elements of both, as well as spanning many components of risk. For example, tobacco control includes individual support to quit, and population wide measures like taxes, regulations around sales and advertising, and road safety spans seat belts, safer cars/roads, drink driving laws and enforcement.
The relationships between the many determinants of health and health outcomes are complex. However, this complexity does provide many potential points of intervention to promote health and reduce the risk of ill health.
Australia’s National Preventive Health Strategy 2021–2030 (NPHS) aims to improve the health and wellbeing of all Australians at all stages of life, through a whole-of-government approach to prevention that addresses the wider determinants of health, reduces health inequities and decreases the overall burden of disease. The NPHS strongly emphasises that preventive action must focus on the wider determinants of health to address the increasing complexity of health issues and the interconnected causes of poor health and wellbeing.
The NPHS contains 4 high-level aims:
- All Australians have the best start in life.
- All Australians live in good health and wellbeing for as long as possible.
- Health equity is achieved for priority populations.
- Investment in prevention is increased (Department of Health 2021).
The AIHW is working to monitor progress against agreed aims and targets in 2024.
The Strategy outlines that the value of prevention is more than preventing disease and promoting a long healthy life. Other benefits include reducing costs:
- of future health care
- for households (such as from tobacco purchases)
- from productivity losses (absenteeism, presenteeism)
- for law enforcement (such as for illicit drug use) (Department of Health 2021).
The Strategy also highlights the importance of monitoring and surveillance in tracking the effectiveness of initiatives, as well as where additional effort may be needed.
Specific determinants
Figure 2 identifies key specific determinants of health. Information on most of these determinants is available in Australia’s health 2024 or other AIHW publications (links below). Two determinants, commercial determinants and health literacy, are not described elsewhere and so are explored further below.
Where to find more information on selected health determinants
Across the specific determinants in Figure 2, detailed information is available in other AIHW reports on:
Broad features of society, including social cohesion, affluence, discrimination
Environmental factors
Socioeconomic characteristics
- Social determinants of health
- Australia’s health 2020 data insights article ‘Social determinants of health in Australia’
- Access to primary health care relative to need for Indigenous Australians
Health behaviours
- Alcohol consumption
- Diet
- Physical activity
- Sleep
- Tobacco and e-cigarettes
- Vaping and electronic cigarette use in Australia in 2022–2023
Psychological factors
Safety factors
- Family, domestic and sexual violence
- Health of people experiencing homelessness
- Health care safety and quality
Biological factors
Commercial determinants of health
What are commercial determinants of health?
Commercial determinants of health (see glossary) are the activities undertaken by commercial organisations that affect people’s health, directly or indirectly, positively or negatively (WHO 2023). An example of a commercial organisation is tobacco companies. Commercial determinants include the systems, practices and pathways through which these organisations affect health and equity (Gilmore et al. 2023).
While private sector commercial organisations can have a positive effect on health (for example, green grocers and gyms), there is a large body of evidence of an increasingly negative effect, particularly linked to multi- and trans-national corporations (Gilmore et al. 2023). Problems can arise when the profit motive conflicts with good health outcomes (Department of Health 2021).
Most focus has been on specific unhealthy products with direct health effects – such as tobacco, alcohol, and discretionary foods – and the large commercial organisations behind them (Lacy-Nichols 2023). However, commercial organisations are diverse, and there is increasing attention being paid to the wider, and more indirect effects. Examples include social media’s effect on mental health and the fossil fuel industry’s contribution to pollution and climate change which in turn harms health (Gilmore et al. 2023).
Changes in the way that people, corporations and governments interact at the international level in recent decades have been identified as enabling health-harming commercial practices. These include:
- The transfer of some public assets to the private sector.
- The rise of transnational corporations which may not be accountable to any one government and have the ability to settle in whichever country serves their interest.
- Available policy options not being used.
- Reductions in government regulations (deregulation) which can remove safeguards against harm (Gilmore et al. 2023; Lacy-Nichols 2023; WHO 2023).
The spectrum of activities commercial organisations engage in ranges from legal and healthy, legal and neutral, legal and harmful, to illegal (Friel et al. 2023).
How do commercial actions affect health?
Commercial organisations can influence health directly or through the broad features of society – by influencing the social, physical and cultural environments. Harms to health are often hidden and indirect, and the many pathways are inter-related.
Commercial determinants can influence health either positively or negatively. The negative impacts causing harm that need to be addressed include:
- product design, packaging and marketing – for example, misleading packaging, inappropriate marketing to children
- supply chains – for example, harm to local communities and the environment during production
- labour and employment – such as low pay levels and dangerous work environments
- reputational management – such as enhancing credibility and corporate image through donating to charity, greenwashing
- research funding and shaping the knowledge environment – for example, influencing the direction and volume of research, spreading unjustified doubt, spreading misinformation and disinformation
- lobbying and donations to influence the political and economic environment – for example, to block or delay regulation that aims to limit harms
- financial practices – including investment in products harmful to health, or tax avoidance
- preference and norms shaping so that their needs are seen as a higher priority than social goods including health – for example, seeking to shape ideas, beliefs and values, funding front groups and think tanks to seed doubt, having supportive media (Department of Health 2021; Gilmore et al. 2023; WHO 2023).
What do we know about the consequences?
The activities of commercial organisations affect many risk factors and health outcomes (Chung et al 2022; UNICEF 2019; WHO 2023). Risk factors include smoking and e-cigarette use, diet, alcohol use, obesity, physical inactivity and air pollution. Health outcomes include acute, chronic and infectious diseases (see glossary) as well as injuries. All groups of society are affected, but the young are particularly vulnerable including through advertising. First Nations people may be disproportionately affected (Maddox et al. 2022). Existing health inequalities are also worsened.
Given the complexity in how commercial determinants can affect health, it is difficult to measure their impact. Using Global Burden of Disease data, it is estimated that 4 commercial products – tobacco, alcohol, ultra-processed food, and fossil fuels – accounted for 19 million global deaths in 2019, which is 34% of all deaths and 41% of non-communicable disease deaths (Gilmore et al. 2023).
An example for one industry – alcohol – illustrates the complexities in commercial determinants.
Location of and access to alcohol outlets
Alcohol causes substantial harm – in Australia in 2022 there were 1,742 alcohol induced deaths and in 2018 it accounted for 4.5% of the total burden of disease (AIHW 2023).
From a public health perspective, the location of and access to alcohol outlets is both an environmental and commercial determinant of health. There is evidence from Australia and internationally showing that living closer to alcohol outlets is associated with increased risky drinking behaviour (Azar et al. 201; Gilmore et al. 2015; Hobbs et al. 2020). Additionally, the number of outlets, days and times of operation, and clustering of outlets are all factors which influence the harms associated with alcohol (Anderson et al. 2009; Livingston et al. 2015; Livingston 2012; Roche et al. 2015).
People living near an alcohol outlet are not only at risk of individual harms from drinking more themselves, but also at risk of alcohol related violence and abuse due to the effect of everyone in their community having greater access to alcohol (AIHW forthcoming 2024). In 2019, people in Capital city areas, estimated to be living within 250 metres of an alcohol outlet, were significantly more likely to have experienced alcohol related harms compared with populations living further away:
- Over 1 in 3 (37%) people drank alcohol in ways that increase the risk of alcohol related disease or injury, compared with 26–30% for people living further away.
- 1 in 4 (25%) people experienced an alcohol related incident like verbal or physical abuse from someone under the influence of alcohol, compared with 12–22% for those living further away.
No relationship between distance and alcohol-related harms was found for people living in non-capital city areas. For all distances, the proportion of people who drank alcohol in ways that increase the risk of alcohol related disease or injury was consistently around 35 to 40%.
This work did not compare across different population groups. Future work could expand upon this analysis to better understand the impact of alcohol outlet locations on different population groups, such as by remoteness and across socioeconomic groups.
Understanding access to alcohol in an area – that is, how close and how many outlets there are – can be used to inform public health and urban planning decisions to reduce the harms from alcohol consumption. Making alcohol less available through control of outlets can reduce harm from alcohol consumption in a cost-effective way (Anderson, et al. 2009).
Health literacy
Health literacy (see glossary) relates to how people access, understand and use health information in ways that benefit their health. People with low health literacy are at higher risk of poorer health behaviours and worse health outcomes.
The idea of health literacy is dynamic and evolving. There are many definitions of health literacy, but they generally share these common elements: health literacy describes the literacy and numeracy skills that enable people to access, understand, assess, and use information to make decisions and take actions that will have an impact on health status (Nutbeam and Lloyd 2021).
Health literacy is needed to:
- Navigate health systems and understand information provided in a healthcare setting and is discussed below in Health literacy in healthcare services.
- Allow people to critically analyse and use information on health determinants from a range of sources such as health advocacy, promotion and consumer engagement (Nutbeam and Lloyd 2021). For more information, see Health promotion and health protection.
Health literacy in healthcare services
Health literacy in the healthcare setting has 2 main components:
- Individual health literacy – these are individual skills, such as the ability to find, understand and use information relevant to health; for example, to complete health care forms or understand and use the health care system.
- The health literacy environment – these are the health system-based elements which need to be considered by health care professionals and organisations, such as policies, processes, and materials, which affect the way the individual engages with the health system (Australian Commission on Safety and Quality in Health Care 2014).
People with low health literacy are more likely to have worse health outcomes overall (Berkman et al. 2011) and adverse health behaviours, such as:
- lower engagement with health services, including preventive services such as cancer screening (Kobayashi et al. 2014)
- higher hospital re-admission rates (Mitchell et al. 2012)
- poorer understanding of medication instructions (for example, non-adherence, improper usage) (Marvanova et al. 2011; Miller 2016)
- lower ability to self-manage care (Geboers et al. 2016).
In contrast, higher levels of health literacy are associated with increased patient involvement in shared decision making (de Oliveira et al. 2018; Seo et al. 2016), which is important in patient-centred care. Improving health literacy is therefore a key element in allowing people to partner with health professionals for better health.
Measuring health literacy
Data generated by measuring health literacy can inform policy decisions and assist health organisations to tailor services appropriately to particular groups of people. The Organisation for Economic Co-operation and Development identified that addressing gaps in health literacy measurement is an important way to remove barriers to health literacy (Moreira 2018). However, the ability to measure health literacy is hampered by the broad range of definitions, a lack of consensus on what to measure, and the multiple approaches to measuring it (Osborne et al. 2013; Poureslami et al. 2017). Data on health literacy in Australia is available from the Health Literacy Survey conducted by the Australian Bureau of Statistics (ABS 2019).
Where do I go for more information?
For more information on determinants of health, see:
- World Health Organisation Commercial determinants of health
- World Health Organisation Determinants of health
- Australian Government Department of Health and Aged Care National Preventive Health Strategy 2021–2030
- AIHW Australia’s health 2020: data insights article ‘Social determinants of health in Australia’.