Australia’s hospitals at a glance
Web article
Last updated:
Topic: Hospitals
Citation
AIHW
Australian Institute of Health and Welfare (2024) Australia’s hospitals at a glance, AIHW, Australian Government, accessed 17 May 2024.
APA
Australian Institute of Health and Welfare. (2024). Australia’s hospitals at a glance. Retrieved from https://www.aihw.gov.au/reports/hospitals/australias-hospitals-at-a-glance
MLA
Australia’s hospitals at a glance. Australian Institute of Health and Welfare, 16 May 2024, https://www.aihw.gov.au/reports/hospitals/australias-hospitals-at-a-glance
Vancouver
Australian Institute of Health and Welfare. Australia’s hospitals at a glance [Internet]. Canberra: Australian Institute of Health and Welfare, 2024 [cited 2024 May. 17]. Available from: https://www.aihw.gov.au/reports/hospitals/australias-hospitals-at-a-glance
Harvard
Australian Institute of Health and Welfare (AIHW) 2024, Australia’s hospitals at a glance, viewed 17 May 2024, https://www.aihw.gov.au/reports/hospitals/australias-hospitals-at-a-glance
The line chart shows that the state and territory governments consistently spent the most on public hospitals whilst non-government entities consistently spent the most on private hospitals.

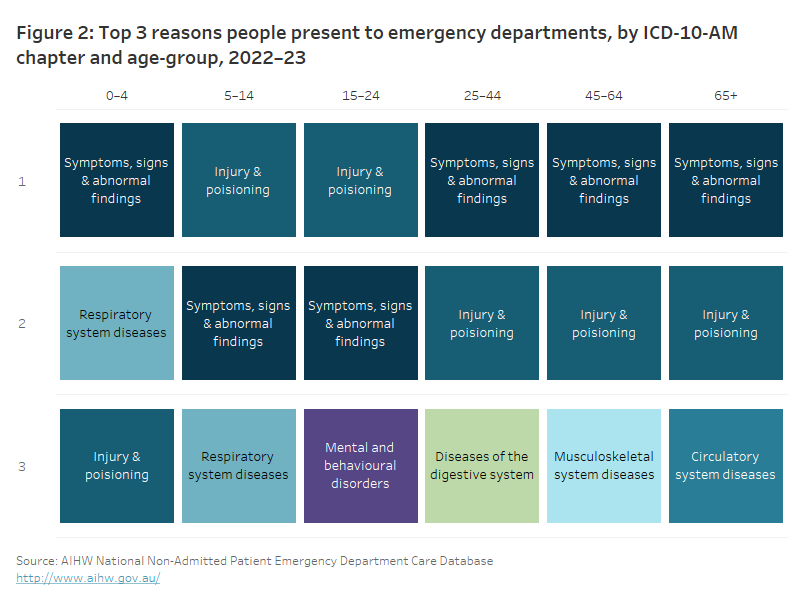
The top reason persons across all age groups present to emergency department is for either ‘Injury and poisoning’ or ‘Symptoms, signs, and abnormal findings’.
The top reason for hospitalisation for both males and females in the age-groups of 45 to 64 and 65+ was for ‘Other factors influencing health status’. ‘Injury and poisoning’ were the top reason for hospitalisation for males in the age groups 5 to 14 and 15 to 24. ‘Pregnancy, childbirth, and the puerperium’ were the top reason for hospitalisation for females in the age-groups 15 to 24 and 25 to 44.

Category 3 which are surgeries that need to be performed within 365 days have the lowest number of admissions throughout the entire financial year compared to category 1 (within 30 days) and category 2 (within 90 days) surgeries. Between December 2022 and February 2023, the number of admissions drops significantly for all clinical urgency categories.

The average length of stay for overnight hospitalisations with a hospital-acquired complication was 21.7 days for public hospitals and 17.1 days for private hospitals. Whilst the average length of stay for overnight hospitalisations without a hospital-acquired complication was 5.1 days for public hospitals and 4.7 days for private hospitals.

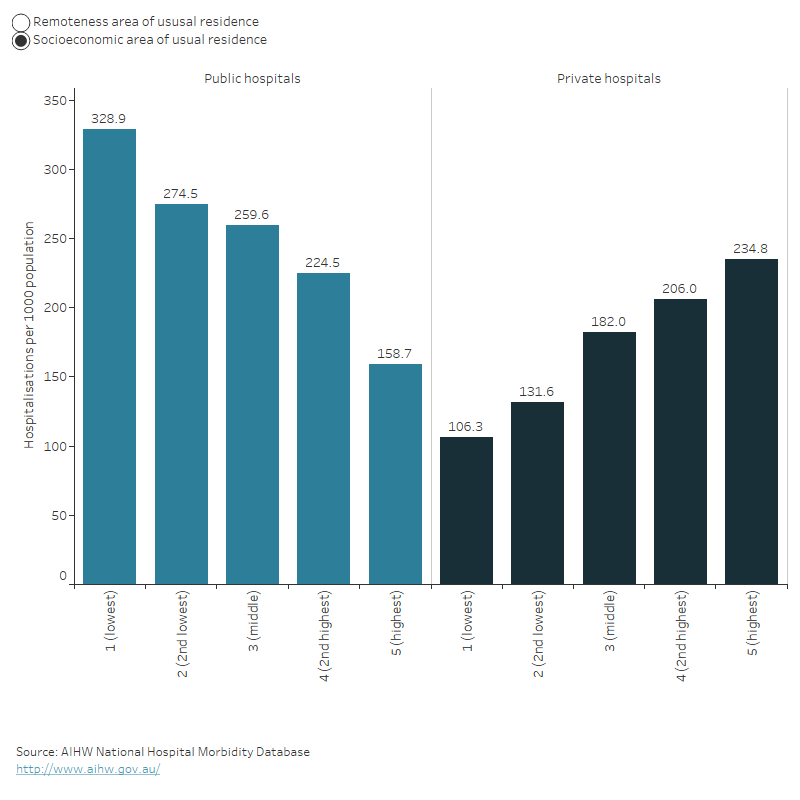
Generally, the number of hospitalisations per 1000 population decreased for public hospitals and increased for private hospitals as the level of disadvantage decreases. Also, the number of hospitalisations per 1000 population generally increased for public hospitals and decreased for private hospitals as the level of remoteness increases.
For more information, see Admitted patient access.
Access to emergency department care
Waiting times
How long people wait in the emergency department before they receive care (waiting time) can be used as a measure of the accessibility of emergency department care.
Waiting time statistics are presented here as:
- the 50th percentile (median) waiting time, which represents the time within which half of all people are seen
- proportion ‘seen on time’ for their triage category.
Emergency department waiting time measures represent the time elapsed from presentation to commencement of clinical care (Figure 7).
Figure 7: Time spent in emergency department

Note: the length of the segments is illustrative only.
Across all emergency presentations to emergency departments in 2022–23, 50% of patients were seen within 20 minutes.
The median waiting time has stayed relatively consistent since 2018–19, when 50% of patients were seen within 19 minutes.
In 2022–23, 65% of presentations to emergency departments were ‘seen on time’.
The proportion of patients seen on time for their triage category has declined slightly since 2021–22 when 67% of patients were seen on time. In 2022–23, the percentage of patients who were seen on time ranged from 100% of patients requiring immediate care (Resuscitation) to 58% of patients who needed care within 30 minutes (Urgent).
In 2022–23, 50% of emergency department presentations were completed within 3 hours and 39 minutes, and 90% were completed within 10 hours and 32 minutes.
For patients who were not subsequently admitted to hospital, 90% completed their care within 7 hours and 19 minutes, but for patients subsequently admitted to hospital, 90% completed their care within 18 hours and 23 minutes.
The time spent in the emergency department for 90% of patients also varied by triage category – ranging from 4 hours and 54 minutes for patients who needed care within 120 minutes (Non-urgent) to 15 hours and 30 minutes for patients requiring immediate care (Resuscitation).
For more information, see Emergency department care access.
Access to surgery
People can be admitted to hospital for emergency surgery, or for less urgent procedures they can be booked in as part of an ‘elective’ (or planned) admission to hospital (elective in this context refers to there being some flexibility around the timing of the procedure, not whether the procedure itself is optional).
Access to surgical services can be affected by issues such as the person’s geographical location, the availability of other healthcare services, and how many people are on public hospital elective surgery waiting lists.
Emergency hospitalisations involving surgery
In 2022–23:
- 382,000 hospitalisations were emergency admissions that involved surgery
- 87% (332,000) were in public hospitals and 13% (49,500) were in private hospitals
- the 3 most common reasons for emergency admissions involving surgery were appendicitis, fractured femur, and heart attack
- people living in Very remote areas were twice as likely to have an emergency admission involving surgery as people living in Major cities (26 compared with 13 hospitalisations per 1,000 population).
Elective hospitalisations involving surgery
In 2022–23:
- 2.5 million hospitalisations were elective admissions involved surgery
- 68% (1.7 million) were in private hospitals and 32% (785,000) were in public hospitals
- the 3 most common reasons for elective admissions involving surgery were cataracts, skin cancer and procreative management
- People living in Major cities were nearly one and a half times as likely to have an elective admission involving surgery as people living in Very remote areas (85 compared with 55 hospitalisations per 1,000 population).
Admissions from public hospital elective surgery waiting lists
In 2022–23, 735,000 patients were admitted for elective surgery from public hospital waiting lists.
Removal of cataracts was the most common procedure (10.3%), followed by Cystoscopy (7.5%). The most common surgical specialty was General surgery (20.3%), followed by Urological surgery (14.6%) and Ophthalmology surgery (13.9%).
For the 25 most common intended procedures in 2022–23, people living in Remote areas had the highest rate of admissions from public hospital elective surgery waiting lists (30 hospitalisations per 1,000 population) followed by people in Inner regional and Outer regional areas (28.3 and 28.2 hospitalisations per 1,000 population respectively). People living in Major cities had the lowest rate of admissions from public hospital elective surgery waiting lists (22 hospitalisations per 1,000 population).
Waiting times for admission to elective surgery
In 2022–23:
- 50% of patients admitted to hospital from public hospital elective surgery waiting lists waited for 49 days or less, and 90% waited for 361 days or less
- 9.6% of people admitted for surgery waited more than 365 days compared to 6.3% just a year before
- 50% of Aboriginal and Torres Strait Islander (First Nations) people were admitted to hospital within 56 days, compared with 50% of non-Indigenous Australians being admitted within 49 days
- the time within which 50% of patients were admitted for their awaited procedure ranged 41 days in Remote areas to 51 days in Outer regional areas for the 25 most common intended procedures
- the time within which 50% of patients were admitted ranged from 31 days for patients living in the highest socioeconomic areas to 14 days for people living in the lowest socioeconomic areas socioeconomic areas for the 25 most common intended procedures.
The 50th percentile waiting time increased from 41 days in 2018–19 to 49 days in 2022–23. The 90th percentile waiting time increased from 279 days in 2018–19 to 361 days in 2022–23.
For more information, see Elective surgery access.
Impact of COVID-19 on hospital care
The COVID-19 pandemic has had an ongoing impact on emergency department, admitted patient and elective surgery activity since its emergence in Australia at the start of 2020.
Impact of COVID-19 on emergency department activity
Emergency department activity in 2019–20, 2020–21 and 2021–22 was influenced by COVID-19 restrictions and the changes affecting health care provision commencing in February 2020. Also, during 2020–21, some jurisdictions operated COVID-19 fever clinics within emergency departments. Comparatively large increases in emergency department activity observed between 2019–20 and 2020–21 in some jurisdictions may be driven, in part, by this additional activity.
Compared with 2018–19, in 2019–20 the number of emergency department presentations decreased by 1.4% – in contrast to the 4.2% increase seen between 2017–18 and 2018–19. In the following year (2020–21) the number of presentations increased by 6.9% – from 8.23 million in 2019–20 to 8.81 million in 2020–21. In 2021–22, the number of presentations decreased by 0.2% to 8.79 million compared with the previous year. Emergency department presentations between 2021–22 and 2022–23, remained relatively stable, increasing by 0.1% overall.
For more information on the impacts of COVID-19 on emergency department activity from 2019–20 to 2022–23, see Emergency department care activity.
Impact of COVID-19 on admitted patient activity
Australia’s hospital system has played a significant role in managing and treating people with COVID-19. Between January 2020 and June in 2023, there were over 454,000 hospitalisations involving a COVID-19 diagnosis (183,400 in 2021–22).
Before the COVID-19 pandemic, there was an upward trend in national hospital admissions, with an average annual increase of 3.3% from 2014–15 to 2018–19. The onset of the pandemic and the ensuing preventative measures resulted in a decrease in hospitalisations in 2019–20 and 2021–22 compared to the respective preceding years. However, in 2022–23, hospitalisations rebounded, showing a 4.6% increase from the previous year, rising from 11.6 million to 12.1 million.
For more information about the impact of COVID-19 on hospital activity and hospitalisations involving COVID-19, see Admitted patient activity.
Impact of COVID-19 on elective surgery activity
As a result of the restrictions on elective surgery introduced in early 2020, overall, there was an 8.3% decrease in elective admissions involving surgery in public hospitals and a 5.7% decrease in private hospitals between 2018–19 and 2019–20.
In addition, there was a 9.2% decrease in admissions from elective surgery waiting lists between 2018–19 and 2019–20.
Delays to elective surgery resulted in a subsequent increase in waiting times for most intended procedures between 2019–20 and 2020–21. The greatest increases in median waiting times occurred for Tonsillectomy (123 day increase over 2019–20), Varicose vein treatment (94 day increase over 2019–20) and Total knee replacement (85 day increase over 2019–20).
The proportion of patients waiting more than 365 days for their elective surgery also increased between 2019–20 and 2020–21 from 2.8% to 7.6% with the greatest increase for Total knee replacement (11% to 32%) and Septoplasty (18% to 36%).
Although, the median waiting times increased in 2022–23, it has decreased for n Cataract extraction (25 days) – from 158 days in 2021–22 to 133 days in 2022–23.
For more information about the impact of COVID-19 on public hospital elective surgery activity, see Elective surgery activity.
Where do I go for more information?
For more information on Australia's hospitals go to MyHospitals.